- Dual GLP-1/Amylin Agonism: Amycretin targets two distinct satiety receptors, delivering synergistic results that outperform traditional mono-agonists like semaglutide.
- Oral Trial Efficacy: 12-week Phase 1 oral clinical trial results show a mean body weight loss of 13.1% with a once-daily pill.
- Subcutaneous Trial Efficacy: 36-week Phase 1b subcutaneous trial results (Dahl et al., 2025) demonstrate dose-dependent weight loss of up to 24.4%.
- Stabilizing Satiety: Amylin co-agonism slows gastric emptying and directly influences hindbrain hunger signaling, effectively eliminating "food noise."
- Manageable GI Profile: Side effects consist mainly of mild-to-moderate nausea and diarrhea, peaking during titration.
- Convenient Oral Option: As a unimolecular agent, oral amycretin represents a long-awaited shift toward needle-free, high-efficacy weight loss.
Introduction: The Paradigm Shift in Medical Weight Management
The landscape of chronic weight management has shifted dramatically over the past decade. Historically, obesity was frequently mischaracterized as a simple behavioral failure—a lack of personal discipline or dietary willpower. However, extensive biochemical research has demonstrated that weight regulation is driven by an intricate network of endocrine signals and neurobiological pathways. The introduction of glucagon-like peptide-1 (GLP-1) receptor agonists, such as semaglutide, marked the beginning of a new era in metabolic medicine. These agents demonstrated that targeting specific hormonal receptors in the brain and digestive tract could achieve significant, sustained weight reduction.
Following the success of GLP-1 mono-agonists, the pharmaceutical industry explored multi-receptor targets. The development of tirzepatide, a dual glucose-dependent insulinotropic polypeptide (GIP) and GLP-1 receptor agonist, proved that activating multiple metabolic pathways simultaneously yields greater weight loss and glycemic control than single-receptor agents. Yet, even with these advances, clinical challenges remain. Weekly subcutaneous injections present barriers for many patients, including "needle anxiety," cold-chain storage logistics, and high manufacturing costs. Furthermore, some patients experience plateaus or find it difficult to tolerate high doses of single-pathway agents.
Enter amycretin, Novo Nordisk's next-generation weight loss agent. Amycretin is a novel, unimolecular co-agonist designed to activate both the GLP-1 receptor and the amylin receptor. This dual-action pathway represents a significant advancement in metabolic research. By targeting two distinct hunger-regulating hormones, amycretin addresses appetite control from multiple anatomical angles. Currently undergoing evaluation in both once-daily oral tablet and once-weekly subcutaneous injection forms, amycretin represents a key milestone in the transition toward highly effective, convenient, and patient-centered weight loss therapies.
The Science of Dual GLP-1/Amylin Receptor Agonism
To understand the clinical potential of amycretin, we must examine the specific physiological mechanisms of GLP-1 and amylin. In a healthy endocrine system, these hormones are secreted from different organs in response to food intake, working together to regulate digestion, glucose levels, and satiety. Targeting both pathways concurrently produces a synergistic effect, amplifying the body's natural satiety signals.
Glucagon-like Peptide-1 (GLP-1) Receptor Pathways
GLP-1 is an incretin hormone synthesized and secreted by the enteroendocrine L-cells of the distal ileum and colon in response to nutrient ingestion. Once released into the portal circulation, GLP-1 exerts its metabolic effects by binding to the GLP-1 receptor (GLP-1R), a G-protein coupled receptor expressed in the pancreas, gastrointestinal tract, and central nervous system. Its primary functions include:
- Glucose-Dependent Insulin Secretion: Binding of GLP-1 to pancreatic beta-cells stimulates adenylate cyclase, increasing intracellular cyclic adenosine monophosphate (cAMP) levels. This cascade activates protein kinase A (PKA) and exchange proteins directly activated by cAMP (such as Epac2), leading to the exocytosis of insulin granules. Crucially, this mechanism is glucose-dependent, minimizing the risk of hypoglycemia.
- Glucagon Suppression: GLP-1 inhibits the secretion of glucagon from pancreatic alpha-cells, which reduces hepatic glucose output and stabilizes fasting blood glucose.
- Slowing Gastric Emptying: In the gastrointestinal tract, GLP-1 activation slows gastric motility. This delays the passage of nutrients into the small intestine, smoothing out postprandial glucose peaks.
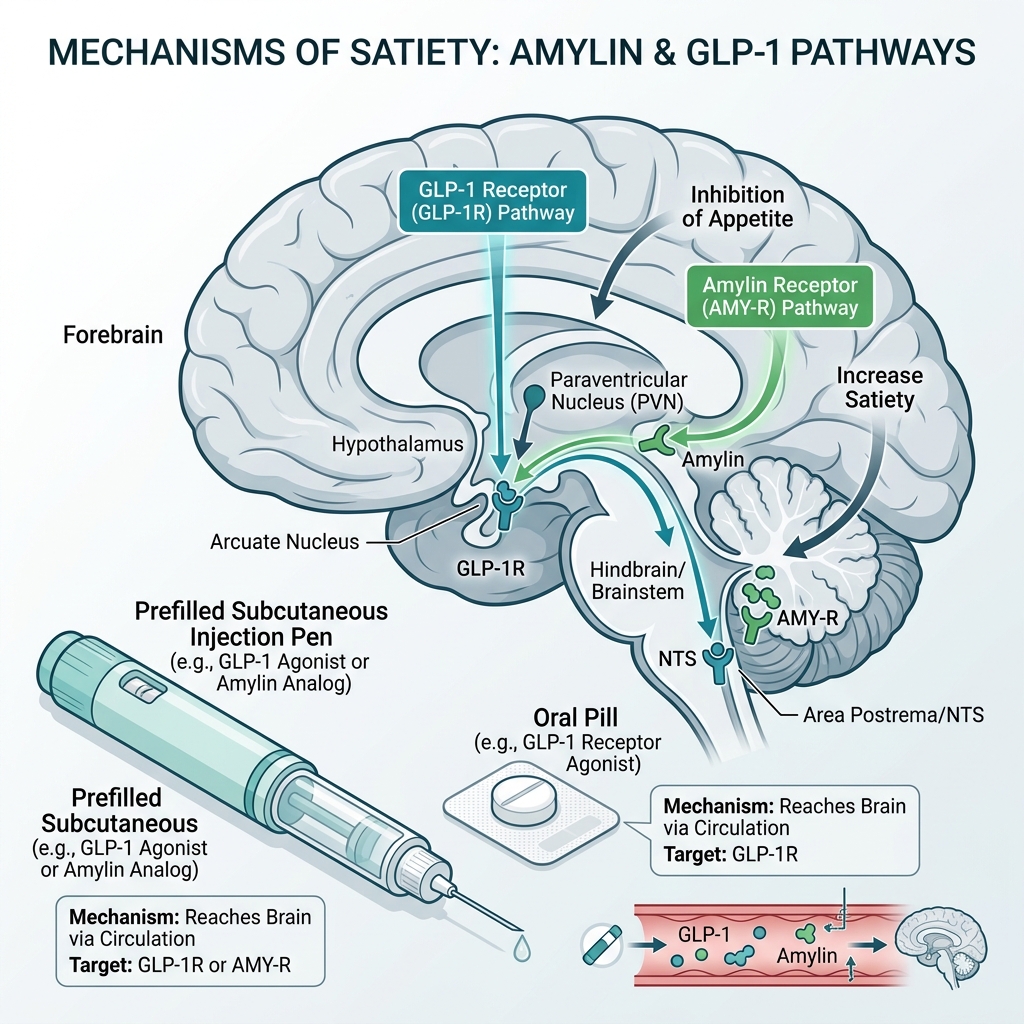
- Hypothalamic Hunger Regulation: In the brain, GLP-1 receptors are highly concentrated in the hypothalamus (specifically the arcuate nucleus). GLP-1 binding stimulates pro-opiomelanocortin (POMC) and cocaine-and-amphetamine-regulated transcript (CART) neurons while inhibiting neuropeptide Y (NPY) and agouti-related peptide (AgRP) neurons. This shifts the central nervous system toward satiety and suppresses overall appetite.
Amylin: The Hindbrain Satiety Signal
Amylin, or islet amyloid polypeptide (IAPP), is a 37-amino-acid peptide hormone that is co-packaged and co-secreted with insulin by pancreatic beta-cells in response to nutrient intake. While insulin regulates glucose disposal in peripheral tissues, amylin acts as a partner hormone to manage nutrient entry into the bloodstream. Unlike GLP-1, which targets the forebrain, amylin's primary site of action is the hindbrain. Its key clinical functions include:
- Satiety Signaling via the Area Postrema: The amylin receptor is a complex molecule consisting of a calcitonin receptor (CTR) core combined with one of three receptor activity-modifying proteins (RAMPs 1, 2, or 3) to form the AMY1, AMY2, or AMY3 receptor subtypes. These receptors are highly expressed in the area postrema (AP), a sensory circumventricular organ in the hindbrain. Activation of the AP signals meal termination, directly reducing meal size and portion volume.
- Complementary Glucagon Inhibition: Amylin suppresses postprandial glucagon secretion via a central pathway, complementing the peripheral pancreatic mechanism of GLP-1.
- Synergistic Gastric Regulation: Amylin slows gastric emptying through vagally mediated pathways, working alongside GLP-1 to prolong gastric distension and sustain physical fullness.
Amylin acts as a primary hindbrain satiety signal. While GLP-1 receptor agonists primarily modulate hunger and reward pathways in the forebrain (hypothalamus), amylin acts on the area postrema in the brainstem to control meal termination and portion size. By targeting both forebrain and hindbrain neurological pathways simultaneously, dual GLP-1/amylin agonists like amycretin generate a synergistic effect that suppresses "food noise" and reduces caloric intake more effectively than mono-agonist therapies.
The Synergy of Co-Agonism
When GLP-1 and amylin receptor pathways are activated simultaneously, their combined effect on weight loss is synergistic rather than additive. GLP-1 receptor activation reduces the drive to eat (hunger) and the reward value of food, while amylin receptor activation accelerates the onset of fullness (satiety) during a meal. By addressing hunger from both the forebrain and the hindbrain, the combination targets the neural networks of appetite control more comprehensively. In preclinical and early clinical studies, this dual activation has shown a powerful reduction in daily caloric intake and food cravings.
Amycretin is engineered as a unimolecular co-agonist—a single peptide chain modified to bind to and activate both the GLP-1 and amylin receptors. This unimolecular design offers significant advantages over co-administering two separate drugs (such as co-formulations of semaglutide and cagrilintide). A single molecule ensures uniform pharmacokinetics, simplifies the manufacturing process, and avoids potential chemical formulation compatibility issues in the syringe or tablet.
Phase 1 Oral Clinical Trial Results
Historically, oral delivery of peptide therapeutics has been a significant challenge in pharmacology. Peptides are highly sensitive to enzymatic degradation by pepsin and other proteases in the stomach and small intestine. Additionally, their large molecular size and hydrophilic nature make it difficult for them to cross the lipid bilayer of the intestinal epithelium. To overcome these barriers, oral amycretin utilizes a proprietary delivery technology developed by Novo Nordisk, which incorporates the absorption enhancer sodium N-[8-(2-hydroxybenzoyl) amino] caprylate (SNAC).
SNAC works by temporarily increasing the local pH in the stomach upon dissolution. This local buffering action protects the amycretin peptide from acid-induced denaturation and proteolytic degradation. Concurrently, SNAC associates with the peptide to facilitate passive transcellular absorption across the gastric mucosa, allowing a therapeutic fraction of the hormone to enter the portal circulation. This is the same technology used in Rybelsus® (oral semaglutide), but it is applied here to a dual-agonist peptide.
The clinical efficacy of once-daily oral amycretin was evaluated in a Phase 1, randomized, double-blind, placebo-controlled, multiple ascending dose (MAD) trial published in The Lancet (Gasiorek et al., 2025). The study enrolled 144 healthy adults with overweight or obesity (BMI of 25.0 to 39.9 kg/m²) who did not have diabetes. Participants were randomized to receive either placebo or oral amycretin, with doses gradually titrated over a 12-week period.
Efficacy and Weight Loss Trajectory
The Phase 1 oral trial demonstrated exceptional efficacy for a short-duration study. Key findings included:
- 13.1% Weight Loss at 12 Weeks: Participants in the highest-dose cohort (who took two 50 mg tablets once daily) achieved an average body weight reduction of 13.1% from baseline at week 12, compared to just 1.1% in the placebo group.
- Dose-Dependent Outcomes: Intermediate dose groups also showed significant weight loss, with the 50 mg single-tablet daily cohort achieving a mean reduction of 10.4% at week 12.
- No Efficacy Plateau: The weight loss curve for oral amycretin remained steep and showed no signs of a plateau at 12 weeks. This trajectory indicates that longer-duration Phase 2 and Phase 3 trials will likely demonstrate even greater cumulative weight loss.
To place these results in context, oral semaglutide (Rybelsus) at its highest approved doses typically yields a 4% to 15% weight loss over a much longer 68-week period, and high-dose oral semaglutide clinical trials (such as OASIS-1) achieved approximately 15% weight loss at 68 weeks. Oral amycretin's ability to achieve a 13.1% reduction in only 12 weeks indicates a highly potent therapeutic profile, driven by the addition of the amylin component.
Because oral peptide absorption is highly sensitive to food and liquid intake, participants in the oral trial followed strict administration rules: taking the tablet in the morning on an empty stomach with a small amount of water (up to 120 ml) and waiting at least 30 minutes before eating, drinking, or taking other oral medications. Adhering to this window is essential to allow the SNAC-mediated absorption process to occur without interference from food particles or excess liquid.
Phase 1b Subcutaneous Study (Dahl et al., 2025)
While the oral formulation of amycretin offers excellent convenience, Novo Nordisk also evaluated a once-weekly subcutaneous injection formulation. Injectable formulations bypass the gastrointestinal tract entirely, avoiding the variable absorption associated with oral administration and ensuring 100% bioavailability. The results of the Phase 1b subcutaneous trial were published in The Lancet by Dahl et al. (2025).
This randomized, double-blind, placebo-controlled, multiple ascending dose trial evaluated once-weekly subcutaneous injections of amycretin in adults with overweight or obesity (without diabetes) over a longer duration of 36 weeks. The study utilized a dose-escalation schedule to evaluate safety, tolerability, pharmacokinetics, and weight-reducing effects across different dose levels.
Weight Loss Results at 36 Weeks
The subcutaneous formulation demonstrated even greater potency than the oral tablet, reflecting the clinical advantages of continuous, systemic exposure. The primary trial outcomes showed:
- Up to 24.4% Weight Reduction: At week 36, participants in the highest dose cohort achieved a mean body weight reduction of up to 24.4%. This represents a massive reduction, average close to one-quarter of initial body weight.
- Rapid Onset: Clinically significant weight loss was visible within the first 4 to 8 weeks of treatment and continued rapidly throughout the 36-week trial.
- Outperforming Current Standards: A 24.4% weight reduction at 36 weeks establishes subcutaneous amycretin as one of the most powerful weight loss agents ever studied. For comparison, Wegovy® (semaglutide 2.4 mg) averages 14.9% weight loss at 68 weeks, and Zepbound® (tirzepatide 15 mg) averages 20.9% weight loss at 72 weeks. Amycretin achieved greater weight loss in roughly half the time.
This rapid weight loss is due to the synergistic interaction of GLP-1 and amylin receptor pathways. By stimulating both receptors via a single peptide, amycretin maintains a strong effect on appetite regulation while potentially reducing the dosage requirements of each component, which can help manage side effects.
It is important to distinguish amycretin from CagriSema, another dual-action pipeline compound from Novo Nordisk. CagriSema is a co-formulation of two separate molecules: semaglutide (a GLP-1 receptor agonist) and cagrilintide (a long-acting amylin analog) mixed in a single injection. While CagriSema is currently in Phase 3 trials and has projected weight loss efficacy of up to 25% over 68 weeks, amycretin is a **unimolecular co-agonist** (a single peptide engineered to target both receptors). A unimolecular design reduces chemical complexity, simplifies manufacturing, and allows for both oral and subcutaneous delivery options.
Explore Affordable Clinical Weight Care Today
While next-generation dual-agonists undergo clinical testing, you can access established, high-efficacy GLP-1 therapies through Losing Weight RX for a flat rate of just $146/month. Take our brief assessment and consult with a provider today.
Get Started OnlineSide Effects and Tolerability Profile
The safety and tolerability of amycretin are critical areas of clinical evaluation. Because both amylin and GLP-1 slow gastric motility and act on central brain regions regulating appetite, the combination of these pathways is expected to result in a standard gastrointestinal (GI) side effect profile. Clinical trial data confirmed this, showing that side effects are consistent with the known pharmacodynamic effects of the individual hormone classes.
Gastrointestinal Adverse Events
In both the oral and subcutaneous trials, the most frequently reported side effects were gastrointestinal, including:
- Nausea: The most common symptom, occurring in a dose-dependent manner. Nausea was typically mild-to-moderate and occurred primarily during the initial titration phase when doses were increased.
- Diarrhea and Vomiting: Reported by a subset of participants, usually resolving within a few days of dose stabilization.
- Constipation: A consequence of slowed gastric emptying and bowel transit. Constipation was generally manageable with hydration and dietary adjustments.
- Decreased Appetite: Although medically classified as an adverse event in early-phase trials, this represents the primary therapeutic mechanism of the drug.
Tolerability During Dosing Titration
A notable finding in the Phase 1 trials was that gastrointestinal side effects were slightly higher during the active titration phase compared to historical GLP-1 mono-agonist trials. This is likely due to the rapid, 12-week titration schedule used in early-phase safety trials to identify maximum tolerated doses. In clinical practice, slower, more gradual titration schedules will be implemented to mitigate these GI effects and allow the gastrointestinal tract to adapt. Slower titration has been shown to reduce both the severity and duration of nausea in patients starting GLP-1 therapies.
The physiological basis of this nausea lies in the dual stimulation of the vagus nerve and the chemoreceptor trigger zone (CTZ) in the brainstem. Both GLP-1 and amylin act on these areas to signal fullness, but rapid increases in concentration can overstimulate the vomiting center. To manage these symptoms during clinical trials, several practical adjustments were helpful:
- Portion Control: Eating smaller, more frequent meals to prevent over-distension of the stomach.
- Dietary Adjustments: Limiting high-fat, greasy, or highly processed foods, which digest slowly and can exacerbate nausea when gastric emptying is delayed.
- Hydration: Maintaining adequate fluid intake throughout the day, particularly with water or electrolyte-rich drinks, to prevent dehydration from diarrhea or vomiting.
- Slower Titration: If side effects become intolerable, clinical protocols often allow patients to remain at a lower dose for an extended period before attempting to escalate again.
Cardiovascular and Pancreatic Safety
Beyond gastrointestinal symptoms, the trials monitored vital signs and laboratory safety parameters. Similar to other GLP-1 receptor agonists, a small, transient increase in resting heart rate (typically 2 to 5 beats per minute) was observed, with no corresponding adverse cardiovascular events. There were no cases of acute pancreatitis, and clinical laboratory values (including amylase and lipase) remained within acceptable boundaries. As a peptide hormone class, amycretin will carry standard warnings regarding the risk of thyroid C-cell hyperplasia and pancreatitis, matching the class profile of semaglutide and tirzepatide.
Clinical Outlook and Projected Timeline (2026 and Beyond)
The clinical development of amycretin highlights a growing trend in obesity medicine: the pursuit of highly effective, needle-free therapies. While subcutaneous injections remain the gold standard for clinical potency, a daily oral pill with high efficacy would eliminate "needle anxiety" and simplify logistics, such as cold-chain shipping and storage. Daily oral administration also aligns naturally with existing daily medication routines, potentially improving long-term patient compliance. However, the choice between oral and subcutaneous formulations will ultimately depend on patient preference and individual metabolic needs.
Novo Nordisk has announced plans to accelerate both the oral and subcutaneous formulations of amycretin into Phase 2 development. In 2026, active Phase 2 trials are evaluating longer-term efficacy, optimal dosing schedules, and safety in broader patient populations (including individuals with Type 2 diabetes and cardiovascular disease). If Phase 2 results match Phase 1 data, global Phase 3 registrational trials will follow.
Under standard drug development timelines, the projected roadmap for FDA approval and commercial launch is estimated around 2028-2029. Until then, patients seeking high-efficacy clinical weight care can utilize existing, proven therapies. Through telehealth platforms like Losing Weight RX, compounded semaglutide remains the most accessible and cost-effective option, offering flat-rate pricing of $146/month without the hidden fees or insurance hurdles of branded injectable products. Compounded options will continue to bridge the clinical gap as next-generation molecules like amycretin complete clinical trials.
Explore Clinical Weight Loss Solutions Today
Take our 5-minute online assessment and consult with a licensed provider within 24 hours to find the right clinical weight loss program for your body, lifestyle, and budget.
Get Started TodayFrequently Asked Questions
Amycretin is a novel, unimolecular dual agonist developed by Novo Nordisk that targets both the GLP-1 (glucagon-like peptide-1) receptor and the amylin receptor. GLP-1 and amylin are complementary metabolic hormones; GLP-1 regulates insulin, suppresses glucagon, and controls hunger in the hypothalamus, while amylin suppresses glucagon, slows gastric emptying, and signals satiety via the area postrema in the hindbrain. This combined pathway produces synergistic weight loss.
In a Phase 1 clinical trial published in The Lancet (Gasiorek et al., 2025), adults taking the highest daily oral dose of amycretin (two 50 mg tablets once daily) lost an average of 13.1% of their body weight in just 12 weeks. This weight reduction is significantly faster than previous oral options like Rybelsus, and the weight loss curve showed no signs of plateauing at 12 weeks.
In a Phase 1b clinical trial published in The Lancet (Dahl et al., 2025), once-weekly subcutaneous injections of amycretin demonstrated a dose-dependent weight loss of up to 24.4% of body weight at 36 weeks in the highest dose cohort. This speed and magnitude of weight reduction exceeds that of currently approved weekly injections such as Wegovy and Zepbound over similar timeframes.
The side effects of amycretin are primarily gastrointestinal, including mild-to-moderate nausea, vomiting, diarrhea, and constipation. These reactions are consistent with other GLP-1 and amylin receptor agonists and are most common during the initial dose titration phase. Slower dose escalation helps mitigate these side effects.
Both amycretin and CagriSema target the GLP-1 and amylin pathways. However, CagriSema is a co-formulation of two separate molecules (semaglutide and cagrilintide) combined in a single injection. Amycretin is a single, unimolecular peptide co-agonist that targets both receptors on its own. This unimolecular design simplifies manufacturing and allows for both oral and subcutaneous delivery options.
Amycretin is currently in Phase 2 clinical development. Following successful Phase 2 trials, it will need to complete larger Phase 3 trials to establish long-term safety and efficacy. Based on standard pharmaceutical development timelines, eventual FDA approval and market launch for either the oral or subcutaneous formulation are projected around 2028-2029.
Clinical References & Sources
- Dahl, K., et al. (2025). Amycretin, a novel, unimolecular GLP-1 and amylin receptor agonist administered subcutaneously: results from a phase 1b/2a randomised controlled study. The Lancet, 405(10492), 244-255. [Lancet Link]
- Khoo, B., & Tan, T. M. (2025). GLP-1 and amylin receptor multiagonism with amycretin for obesity management. The Lancet, 405(10492), 201-203. [Lancet Link]
- Gasiorek, A., Heydorn, A., et al. (2025). Safety, tolerability, pharmacokinetics, and pharmacodynamics of the first-in-class GLP-1 and amylin receptor agonist, amycretin: a first-in-human, phase 1, double-blind, randomised, placebo-controlled trial. The Lancet, 406(10499), 135-148. [Lancet Link]