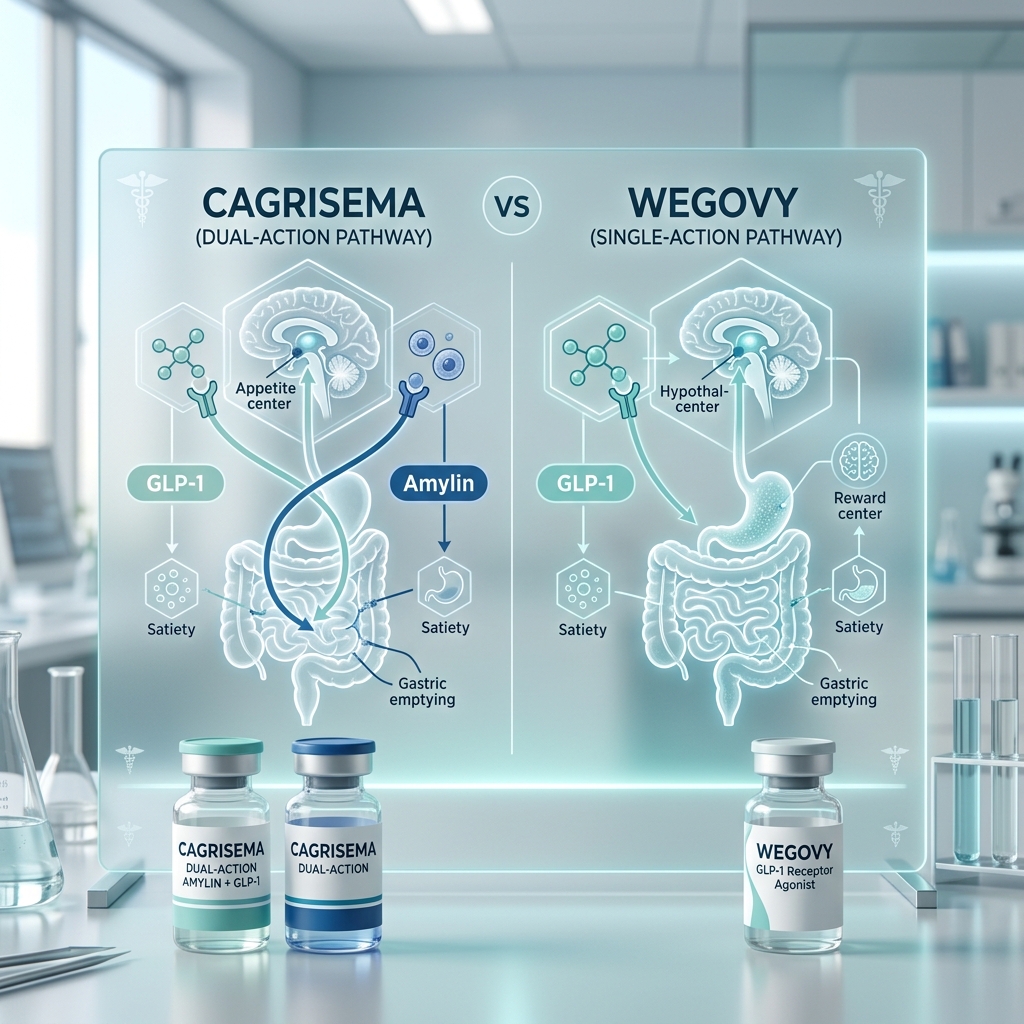
- Dual-Action Mechanism: While Wegovy targets only the GLP-1 pathway, CagriSema combines semaglutide with cagrilintide (a long-acting amylin analogue) to target two distinct neurochemical appetite pathways.
- Phase 2 Superiority: In clinical trials for patients with type 2 diabetes and obesity, CagriSema achieved an average weight loss of 15.6% in 32 weeks, significantly outperforming Wegovy monotherapy which achieved 5.1% in the same cohort.
- Bariatric-Level Efficacy: Projected Phase 3 trial results (the REDEFINE program) for CagriSema indicate weight loss outcomes in the 20% to 25% range, representing a new peak in pharmaceutical obesity medicine.
- Side Effect Profiles: CagriSema carries a similar side effect profile to Wegovy—mostly transient, mild-to-moderate gastrointestinal events—though gastrointestinal symptoms are slightly more frequent during titration.
- Approval & Access: Wegovy is FDA-approved and widely available. CagriSema is currently in Phase 3 trials with regulatory decisions expected by late 2026 or 2027.
Introduction: The Next Frontier in Obesity Medicine
The landscape of medical weight management has undergone a historic transformation over the last five years. The introduction of glucagon-like peptide-1 (GLP-1) receptor agonists, spearheaded by semaglutide (approved for weight loss as Wegovy®), established a new baseline for what anti-obesity medications could achieve. Historically, older generations of weight loss drugs achieved modest body weight reductions of 5% to 8%, often accompanied by unfavorable safety profiles. Wegovy changed that paradigm by demonstrating an average weight reduction of approximately 15% in landmark clinical trials.
However, the pharmaceutical landscape does not stand still. As research into metabolic endocrinology accelerates, scientists have turned their focus from single-hormone therapies to multi-receptor agonists and combinations. The goal is to safely mimic the complex, multi-hormonal signaling that occurs naturally in the human body after food consumption. In this quest for superior efficacy, Novo Nordisk has developed CagriSema, a novel fixed-dose combination therapy designed to challenge both standard monotherapies like Wegovy and dual-receptor competitors like tirzepatide (Zepbound®).
This clinical review provides an in-depth comparison of CagriSema vs Wegovy. We will analyze the underlying biological mechanisms, review the published clinical trial results, examine side effect profiles, outline titration schedules, and discuss the FDA approval timeline. Understanding the evidence behind these two therapies is critical for patients and providers navigating the future of chronic weight management.
Understanding Wegovy: The Monotherapy Standard
To understand the clinical significance of CagriSema, it is first necessary to examine the mechanism and trial data of Wegovy. Wegovy is a once-weekly subcutaneous injection of semaglutide at a maintenance dose of 2.4 mg. Semaglutide is a synthetic analog of human GLP-1, a hormone naturally secreted by the L-cells of the small intestine in response to nutrient intake.
The physiological actions of Wegovy are mediated through three primary systems:
- Central Appetite Regulation: Semaglutide crosses the blood-brain barrier to act directly on the arcuate nucleus of the hypothalamus. It stimulates pro-opiomelanocortin (POMC) neurons (which promote satiety) and inhibits neuropeptide Y/agouti-related peptide (NPY/AgRP) neurons (which stimulate hunger). The clinical result is a significant decrease in appetite and a reduction in "food noise"—the intrusive, obsessive thoughts about eating that characterize the pathology of obesity.
- Gastric Motility: Wegovy slows gastric emptying, delaying the transit of food from the stomach to the duodenum. This prolongs postprandial satiety, physically maintaining the sensation of fullness for an extended period.
- Glycemic Optimization: Semaglutide stimulates glucose-dependent insulin secretion from pancreatic beta cells while simultaneously suppressing glucagon secretion from alpha cells. This improves insulin sensitivity and glycemic control without inducing hypoglycemia.
The clinical efficacy of Wegovy was established through the landmark STEP (Semaglutide Treatment Effect in People with obesity) clinical trial program. In the STEP-1 trial, a 68-week, double-blind, placebo-controlled study involving 1,961 adults without diabetes, participants taking Wegovy achieved a mean body weight loss of 14.9% from baseline, compared to just 2.4% in the placebo group. Furthermore, 32% of participants on Wegovy achieved a body weight loss of 20% or more. This level of efficacy established Wegovy as the gold standard of GLP-1 monotherapy, demonstrating metabolic improvements in blood pressure, lipid profiles, and inflammatory markers like high-sensitivity C-reactive protein (hs-CRP).
Understanding CagriSema: The Dual-Action Combination
While Wegovy targets a single hormonal pathway, CagriSema utilizes a dual-action mechanism. CagriSema is a fixed-dose combination containing two distinct active pharmaceutical ingredients: semaglutide (2.4 mg) and cagrilintide (2.4 mg), administered together in a single weekly injection. Cagrilintide is a novel, long-acting analogue of amylin, a pancreatic hormone that works in concert with GLP-1 but operates through entirely distinct physiological pathways.
The Role of Amylin in Appetite Regulation
Amylin is a 37-amino acid peptide hormone co-secreted with insulin by the pancreatic beta cells in response to meals. While insulin primarily regulates glucose disposal into peripheral tissues, amylin acts as a neuroendocrine regulator of energy balance. It binds to amylin receptors in the hindbrain, specifically in the area postrema (AP) and the nucleus tractus solitarius (NTS). Through these hindbrain pathways, amylin signals homeostatic satiety, reduces gastric acid secretion, and slows gastric emptying.
Because amylin and GLP-1 act on different regions of the central nervous system—amylin predominantly in the hindbrain (area postrema) and GLP-1 in both the hindbrain and the hypothalamus—combining them offers a powerful synergistic effect. Rather than simply increasing the dose of a single hormone (which eventually hits a therapeutic plateau and increases side effects), combining semaglutide with cagrilintide recruits two distinct neural circuits to regulate energy intake. This multi-pathway activation targets the complex, redundant biological systems that protect body weight set points during caloric restriction.
GLP-1 Pathway (Semaglutide)
Acts on the hypothalamus and hindbrain to promote satiety, decrease hunger, and turn down mental "food noise." It also slows gastric emptying and optimizes pancreatic insulin secretion.
Amylin Pathway (Cagrilintide)
Acts directly on the hindbrain (area postrema) to signal fullness, suppress glucagon release, and delay gastric transit. Operates independently of and complementarily to the GLP-1 pathway.
In obesity pharmacotherapy, synergy means the combination of two drugs produces a clinical effect greater than the sum of their individual parts. By targeting both the hypothalamus (GLP-1) and the hindbrain (amylin), CagriSema achieves profound appetite regulation at lower relative doses, maximizing weight loss while managing the side-effect profile.
CagriSema vs Wegovy: Clinical Trial Results
The primary clinical evidence comparing CagriSema and Wegovy comes from a randomized, double-blind, active-controlled Phase 2 clinical trial published in The Lancet. This trial evaluated the efficacy and safety of the combination vs. its monotherapy components in adults with type 2 diabetes and obesity (a patient population traditionally known for slower and less pronounced weight loss compared to cohorts without diabetes).
The Phase 2 Trial Design and Efficacy Data
The 32-week trial randomized 277 participants into three main treatment arms:
- CagriSema Arm: Fixed-dose combination of cagrilintide 2.4 mg + semaglutide 2.4 mg once weekly.
- Semaglutide Monotherapy Arm (Wegovy equivalent): Semaglutide 2.4 mg once weekly.
- Cagrilintide Monotherapy Arm: Cagrilintide 2.4 mg once weekly.
At the end of the 32-week treatment period, the differences in weight loss and metabolic outcomes were stark:
- Mean Body Weight Loss: Participants in the CagriSema group achieved an average weight loss of 15.6% of their initial body weight. In contrast, those in the semaglutide monotherapy group lost 5.1%, and those in the cagrilintide monotherapy group lost 8.1%. The combination therapy resulted in more than triple the weight loss of Wegovy monotherapy in this diabetic population.
- Glycemic Control (HbA1c Reduction): Glycemic control is a key metric for patients with diabetes. CagriSema reduced HbA1c levels by a mean of 2.2 percentage points. This was significantly superior to the reductions seen with semaglutide alone (1.8 percentage points) and cagrilintide alone (1.3 percentage points).
- Satiety Metrics: Patient-reported outcome measures indicated a substantially greater decrease in cravings and hunger scores in the CagriSema group compared to either monotherapy, confirming the synergistic action of the two pathways.
| Clinical Metric | Wegovy (Semaglutide 2.4 mg) | CagriSema (Semaglutide 2.4 mg + Cagrilintide 2.4 mg) | Clinical Significance |
|---|---|---|---|
| Active Receptors | GLP-1 receptor only | GLP-1 & Amylin receptors | CagriSema targets two distinct appetite areas of the brain. |
| Phase 2 Weight Loss (32 Wks) | 5.1% (in T2D cohort) | 15.6% (in T2D cohort) | More than 3x the weight loss in comparative diabetic trials. |
| Projected Weight Loss (68 Wks) | ~15% (non-diabetic cohort) | 20% to 25% (projected) | Expected to equal or exceed Zepbound (tirzepatide) efficacy. |
| HbA1c Reduction (T2D) | -1.8% | -2.2% | CagriSema shows superior glycemic control for diabetics. |
| Administration | Once-weekly subcutaneous injection | Once-weekly subcutaneous injection | Both use standard weekly injection protocols. |
| FDA Approval Status | Approved (since 2021) | In Phase 3 clinical trials | Wegovy is widely available; CagriSema is pending approval. |
Understanding the REDEFINE Phase 3 Trial Program
Following the successful Phase 2 results, Novo Nordisk initiated the extensive REDEFINE Phase 3 clinical trial program. The REDEFINE program consists of several large-scale global trials designed to establish the safety, efficacy, and cardiovascular outcomes of CagriSema across diverse patient populations:
- REDEFINE 1 (NCT05567796): A 68-week trial evaluating CagriSema vs. semaglutide monotherapy, cagrilintide monotherapy, and placebo in approximately 3,400 adults with obesity or overweight without diabetes. This is the pivotal trial expected to establish CagriSema's primary weight management label. Efficacy projections indicate mean weight loss could reach or exceed 20% to 25%, establishing CagriSema clinical trial results as some of the most potent in medical history.
- REDEFINE 2 (NCT05394571): A 68-week trial evaluating the safety and efficacy of CagriSema compared to placebo in adults with obesity and type 2 diabetes. This study will expand upon the Phase 2 glycemic and weight loss data.
- REDEFINE 3 (NCT05668585): A cardiovascular outcomes trial (CVOT) designed to assess whether CagriSema reduces major adverse cardiovascular events (MACE), such as cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke, in patients with obesity and established cardiovascular disease. This trial is critical for establishing long-term safety benefits similar to those demonstrated by Wegovy in the SELECT cardiovascular outcomes trial.
Begin Your Weight Loss Program with Semaglutide for $146/mo
While next-generation combinations undergo FDA trials, you can access the proven weight loss power of compounded semaglutide today. Flat-rate pricing at all dosage levels with free shipping.
Start Your AssessmentSide Effects and Safety Profiles: A Comparative View
A critical consideration in evaluating a dual-hormone combination is whether the addition of a second compound increases side effects. In the clinical trials published to date, the side effect profile of CagriSema was consistent with what is typically observed with Wegovy, consisting primarily of mild-to-moderate gastrointestinal events. However, because both compounds delay gastric transit through separate pathways, gastrointestinal side effects did occur at slightly higher rates during titration.
Gastrointestinal Side Effects
The most common side effects reported in both the Wegovy and CagriSema clinical cohorts include:
- Nausea: Nausea remains the most frequently reported side effect for both medications. In the Phase 2 trial, nausea occurred in approximately 40% to 50% of patients taking CagriSema, slightly higher than or comparable to Wegovy. The severity of nausea was classified as mild to moderate and occurred mostly during the dose-escalation phase.
- Constipation and Diarrhea: Both bowel changes are common. Diarrhea tends to occur more frequently in the early stages of treatment, while constipation can persist longer due to the continuous delay in gastric emptying.
- Vomiting and Dyspepsia: These symptoms were closely associated with dietary composition. Eating high-fat meals or eating past the point of initial satiety triggers these symptoms more readily in patients on dual-action therapies.
Serious Clinical Safety and Warnings
Because CagriSema contains semaglutide, it carries the same class-wide safety warnings as Wegovy, including:
- Thyroid C-Cell Tumor Risk: In rodent studies, semaglutide caused a dose-dependent increase in thyroid C-cell tumors. While it is unknown if this occurs in humans, CagriSema and Wegovy are contraindicated in patients with a personal or family history of Medullary Thyroid Carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2).
- Pancreatitis: Acute pancreatitis has been reported in clinical trials of GLP-1 receptor agonists. Patients should immediately discontinue therapy if they experience severe, persistent abdominal pain radiating to the back.
- Gallbladder Disease: Rapid weight loss is associated with an increased incidence of cholelithiasis (gallstones) and cholecystitis. In clinical trials, gallbladder-related events occurred at similar rates between Wegovy and CagriSema.
- Hypoglycemia Risk: When used in combination with an insulin secretagogue (like a sulfonylurea) or insulin, the risk of low blood sugar increases. Doses of these concomitant medications may need to be adjusted.
Titration, Administration, and Dosing Schedules
To safely manage the side effects of both medications, a structured titration schedule is required. Titration allows the gastric and neurological systems to adjust to the exogenous hormonal signaling gradually. Once-weekly subcutaneous injections are self-administered in the abdomen, thigh, or upper arm on the same day each week.
Wegovy Dosing and Titration
Wegovy follows a standard 16-week titration protocol to reach the 2.4 mg maintenance dose:
CagriSema Dosing and Titration
CagriSema is formulated as a fixed-dose combination in a single injector pen. Based on clinical trial designs, the titration schedule is expected to mirror the standard semaglutide titration, gradually increasing both the semaglutide and cagrilintide components in tandem. The targeted maintenance dose evaluated in trials is 2.4 mg semaglutide paired with 2.4 mg cagrilintide. Patients will start at the lowest combination dose (0.25 mg / 0.25 mg) and scale upward over a period of 16 to 20 weeks. This slow ramp-up is designed to mitigate the combined gastrointestinal effects of the two active ingredients.
FDA Approval Status and Timeline (2026)
When comparing Wegovy and CagriSema, availability is a key clinical distinction. Wegovy received FDA approval for chronic weight management in June 2021, and its cardiovascular risk reduction label was approved in early 2024. Consequently, Wegovy is fully commercialized and available in retail pharmacies, though it has faced supply shortages due to unprecedented consumer demand.
In contrast, CagriSema is not yet approved by the FDA. The drug is currently in Phase 3 clinical trials, with the REDEFINE program expected to yield definitive results throughout late 2025 and 2026. Novo Nordisk has prioritized CagriSema as a cornerstone of its obesity pipeline, aiming to submit its New Drug Application (NDA) to the FDA as soon as the pivotal REDEFINE 1 study is completed. This timeline suggests that CagriSema FDA approval and subsequent market entry could occur in late 2026 or early 2027, depending on regulatory review speed. Until then, Wegovy and tirzepatide remain the only approved high-potency weight loss injectables on the market.
Clinical Decision Matrix: Wegovy vs. CagriSema
Once both therapies are clinically available, how should providers and patients choose between them? The choice will depend on clinical history, weight loss goals, tolerability, and access.
Wegovy is the preferred clinical option for:
- First-Line Therapy: Patients starting GLP-1 weight loss therapy for the first time. Wegovy has a well-established safety profile, with long-term real-world safety data from millions of patients.
- Insurance Coverage: Because Wegovy is established, it has broader insurance coverage and formulary placement, making it more affordable for patients with employer-sponsored plans.
- Moderate Weight Loss Goals: Patients aiming to lose 10% to 15% of their body weight to resolve metabolic health conditions.
CagriSema is expected to be the preferred option for:
- GLP-1 Responders with Plateaus: Patients who have hit a weight loss plateau on Wegovy or tirzepatide but still require further weight loss to achieve their clinical goals. The addition of the amylin pathway can re-sensitize appetite centers and restart weight loss.
- Bariatric-Level Requirements: Patients with severe obesity (BMI > 40) who require substantial weight reductions of 20% to 25% or more but wish to avoid the surgical risks of gastric bypass or sleeve gastrectomy.
- Severe Type 2 Diabetes Management: Diabetics with poorly controlled HbA1c who require maximum glycemic optimization and significant cardiovascular risk reduction.
Cost, Access, and Compounding Considerations
The cost of anti-obesity medications is a significant barrier for many patients. Wegovy lists at approximately $1,349 per month without insurance. Because many insurance plans exclude obesity treatments from coverage, patients are often forced to pay out-of-pocket or seek alternative access routes. When CagriSema enters the market, it is expected to carry a premium price, likely equal to or higher than Wegovy's current list price, making out-of-pocket access extremely challenging.
To address these cost barriers, many patients turn to compounded GLP-1 medications. Compounding pharmacies can prepare semaglutide using the same active pharmaceutical ingredient under Section 503A of the Federal Food, Drug, and Cosmetic Act. Through telehealth platforms like Losing Weight RX, patients can access compounded semaglutide for a flat rate of $146 per month, regardless of the dose level. This represents a savings of nearly 90% compared to brand-name Wegovy, providing a clinically effective pathway to weight loss without the financial strain of retail brand pricing.
Once CagriSema receives FDA approval, it will remain under patent protection for years, preventing standard generic versions from entering the market. While traditional compounding pharmacies can prepare individual semaglutide prescriptions, compounding a complex combination like CagriSema requires specialized manufacturing that may not be immediately available through 503A pharmacies, making early access to CagriSema highly dependent on commercial insurance coverage.
Frequently Asked Questions
CagriSema is not a single molecule; it is a fixed-dose combination of two different active molecules. One component is semaglutide, which is the identical active ingredient in Wegovy. The second component is cagrilintide, a novel long-acting amylin analogue. While Wegovy contains only semaglutide, CagriSema combines it with cagrilintide to achieve a dual-action appetite-regulating effect that targets two separate pathways in the brain.
Yes. Published clinical data from a Phase 2 trial in patients with type 2 diabetes and obesity showed that CagriSema led to a mean body weight reduction of 15.6% after 32 weeks, compared to only 5.1% for the semaglutide monotherapy group (Wegovy equivalent). In ongoing Phase 3 trials in patients without diabetes, CagriSema is projected to achieve average weight loss results in the 20% to 25% range, significantly outperforming Wegovy monotherapy.
CagriSema is currently in Phase 3 clinical testing under the REDEFINE clinical trial program. Key efficacy and safety data from these pivotal trials are expected to be published throughout late 2025 and 2026. Depending on the trial outcomes and FDA review times, official CagriSema FDA approval could occur in late 2026 or 2027. Wegovy remains approved and available today.
In Phase 2 trials, CagriSema's overall safety and tolerability profile was comparable to Wegovy. The most common side effects for both are gastrointestinal, including nausea, diarrhea, constipation, and vomiting. However, because CagriSema combines two different mechanisms that delay gastric transit, gastrointestinal side effects occurred at slightly higher rates during titration in the combination group. Most symptoms were mild to moderate and resolved over time.
Both medications are administered once weekly as a subcutaneous injection. CagriSema is co-formulated into a single fixed-dose injection, meaning patients only need to perform one injection per week, identical to the administration process for Wegovy. Both are typically injected into the abdomen, thigh, or upper arm on the same day each week, with or without food.
Yes, switching will be clinically feasible under provider supervision. Switching is expected to be a primary clinical pathway for patients who have plateaued on Wegovy or other GLP-1 medications but still require further weight reduction. Your provider will establish a safe transition protocol, which may involve starting at a lower combination dose of CagriSema to ensure gastrointestinal tolerance.
Start Compounded Semaglutide for $146/mo Flat-Rate
Skip the insurance hurdles and high out-of-pocket costs of brand-name Wegovy. Complete our brief online assessment to get evaluated by a licensed U.S. provider and receive your medication from a licensed 503A pharmacy.
Get Started TodayClinical References & Sources
- Frias, J. P., Davey, P., et al. (2023). Efficacy and safety of co-administered cagrilintide and semaglutide (CagriSema) in type 2 diabetes: a multicentre, randomised, double-blind, active-controlled, phase 2 trial. The Lancet, 402(10403), 720-730. Lancet Journal Link
- Wilding, J. P. H., Bateman, A. H., et al. (2021). Once-weekly semaglutide in adults with overweight or obesity. New England Journal of Medicine, 384(11), 989-1002. ClinicalTrials.gov (NCT03548935)
- Novo Nordisk. (2024). A research study to look at how well CagriSema works compared to semaglutide, cagrilintide and placebo in people with overweight or obesity (REDEFINE 1). ClinicalTrials.gov (NCT05567796)
- Novo Nordisk. (2024). A research study to compare the effect of CagriSema once-weekly versus placebo once-weekly on body weight in people with type 2 diabetes and overweight or obesity (REDEFINE 2). ClinicalTrials.gov (NCT05394571)