- Defining Food Noise: Food noise is the constant, intrusive, and obsessive thoughts about food, eating, and cravings that occupy a person's mental space, driving eating patterns independently of actual caloric needs.
- The Dopaminergic Effect: Semaglutide targets GLP-1 receptors in the mesolimbic dopamine pathway, effectively dampening the neurological reward response associated with highly palatable foods.
- Biological vs. Emotional Hunger: While GLP-1 receptor agonists eliminate physical hunger and silence food noise, they do not resolve underlying emotional triggers such as stress, boredom, anxiety, depression, or trauma.
- CBT Integration is Essential: Cognitive Behavioral Therapy (CBT) and mindful eating interventions are vital during GLP-1 therapy to build non-food coping mechanisms and behavioral strategies.
- Discontinuation Preparedness: If semaglutide is titrated down or stopped, biological food noise will return; developing psychological tools while on the drug is the key to preventing rebound weight gain.
1. The Revolution of GLP-1 Therapy and the Eating Behavior Paradigm
The introduction of glucagon-like peptide-1 (GLP-1) receptor agonists, specifically semaglutide (available under brand names like Ozempic® and Wegovy® or as compounded formulations), has fundamentally shifted the clinical treatment of obesity and metabolic syndrome. In the past, weight loss interventions focused almost exclusively on willpower and strict dietary restraint—approaches that clinical research has consistently shown fail for the vast majority of patients with chronic metabolic disease. By mimicking a natural gut hormone, semaglutide targets physiological systems to suppress appetite and delay gastric emptying, providing a powerful biological tool for weight management.
However, as clinicians gain experience with these medications, a critical realization has emerged: weight management is not solely a physiological challenge. Eating is deeply intertwined with human psychology, emotional regulation, and neurobiology. While semaglutide is remarkably effective at correcting metabolic dysfunction, reducing physical hunger, and silencing obsessive food thoughts, it does not rewrite a patient's emotional history or automatically establish healthy coping mechanisms. Patients who have spent years using food as a primary tool to manage stress, loneliness, anxiety, or trauma frequently discover that while their physical capacity to consume large volumes of food has decreased, the psychological urge to eat in response to emotions remains active. To optimize long-term health, patients must address both the biological and psychological dimensions of their relationship with food.
2. Understanding "Food Noise" and Its Neurobiological Drivers
To understand how semaglutide alters eating behavior, one must first define a phenomenon that patients and clinicians refer to as "food noise." In clinical terms, food noise represents the constant, intrusive, and obsessive thoughts about food, cravings, and eating that dominate a person's mental space. It is not simply the feeling of physical hunger; rather, it is a persistent cognitive background track that prompts questions like: *When will I eat next? What will I eat? How much is left in the pantry? Can I justify having that snack right now?* For individuals with a high level of food noise, these thoughts can be exhausting, distracting, and incredibly difficult to override with cognitive control alone.
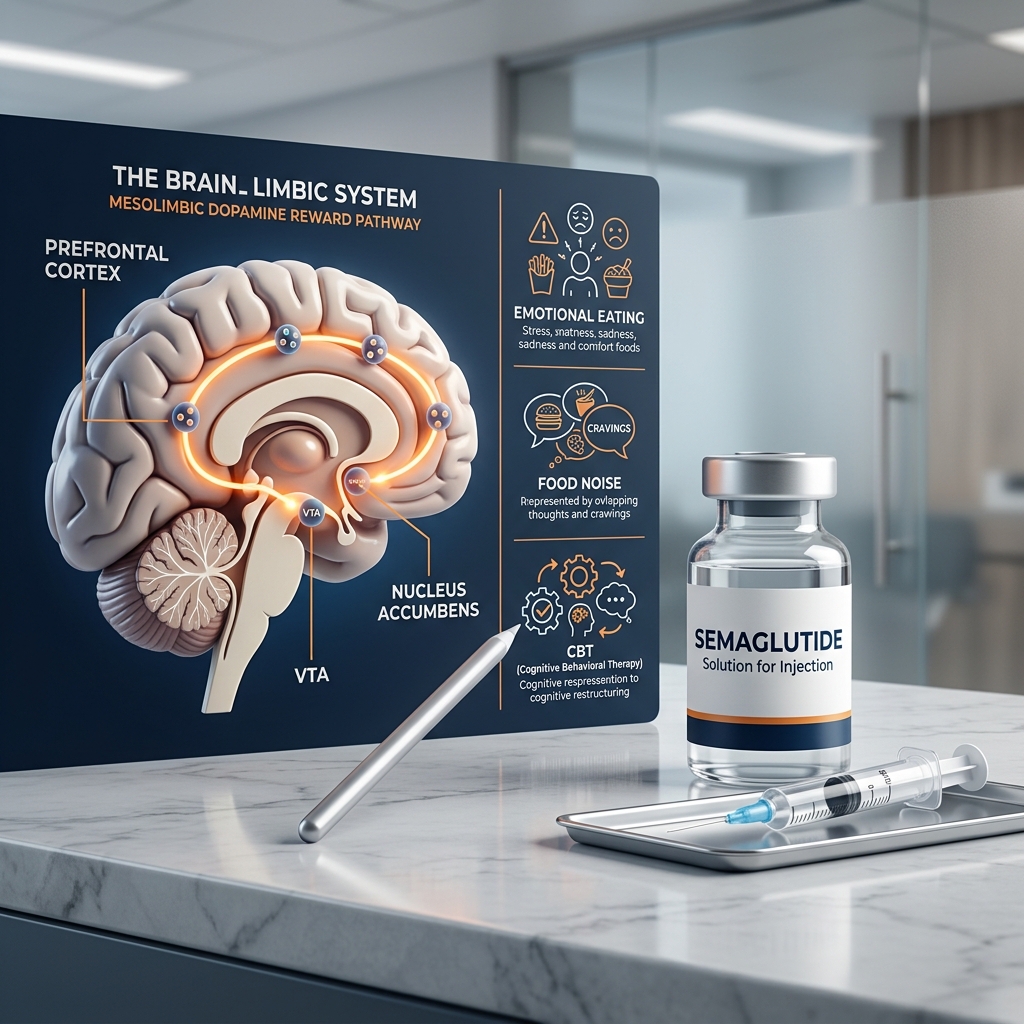
From a neurobiological perspective, food noise is driven by hyperactive signaling in the brain's reward centers. In the human brain, eating is regulated by two distinct systems: the homeostatic system (which monitors energy balance and nutritional needs) and the hedonic system (which monitors pleasure and reward). The hedonic system is centered in the mesolimbic dopamine pathway—often called the brain's reward circuit. When we consume highly palatable foods (those high in sugar, fat, and salt), the brain releases dopamine, a neurotransmitter that signals pleasure and reinforces the behavior. In individuals with obesity or genetic predispositions to food addiction, this reward pathway can become sensitized, requiring greater stimulation to achieve satisfaction and triggering intense, compulsive cravings. This neurological drive manifests subjectively as food noise.
3. How Semaglutide Rewires Cravings in the Brain's Reward System
Semaglutide is a long-acting peptide that mimics the endogenous hormone GLP-1. While it is well-known for its actions in the pancreas (stimulating glucose-dependent insulin secretion) and the stomach (slowing gastric emptying), its most profound effects on food noise occur within the central nervous system. Semaglutide is structurally modified to resist rapid enzymatic breakdown, enabling it to cross the blood-brain barrier and access key neurological targets.
Specifically, semaglutide binds to GLP-1 receptors in the hypothalamus, the area postrema, and the mesolimbic dopamine pathway. By activating these receptors, semaglutide alters the brain's neurochemistry in several critical ways:
- Dampening Dopaminergic Reward: Semaglutide directly dampens the release of dopamine in the nucleus accumbens in response to highly palatable foods. When the reward response is muted, the expectation of pleasure from eating decreases. A slice of cake or a bag of chips no longer triggers the same intense neurological "high," which lowers the incentive to seek out these foods.
- Reducing Reward-Driven Impulse: By regulating the mesolimbic pathway, semaglutide helps restore cognitive control over food intake. Patients often report that they can look at their favorite foods and decide, without effort or anxiety, to walk away. The drug effectively decreases impulsivity and enhances executive function within the prefrontal cortex relative to eating decisions.
- Satiating the Hedonic Appetite: The drug mimics a state of constant energy abundance, tricking the brain into believing that metabolic needs are fully met. This silences the hedonic drive to eat for pleasure, effectively turning off the mental chatter of food noise.
This neurochemical shift explains why patients on semaglutide often experience a profound sense of peace. The mental energy previously consumed by resisting cravings is suddenly freed up, allowing them to establish a more neutral, functional relationship with food. It is highly recommended to follow a structured, nutrient-dense diet during this quiet period, as detailed in our guide on the ideal semaglutide diet plan.
Compounded Semaglutide at a Flat $146/Month
Quiet the food noise and reclaim control of your metabolic health. Get evaluated online by a licensed U.S. medical provider and receive sterile compounded semaglutide shipped directly to your door. Flat-rate pricing at all dosage levels.
Start Your Assessment4. The Crucial Disconnect: Physiological Hunger vs. Emotional Hunger
While semaglutide is incredibly effective at regulating the biological signaling of hunger and reward, it is not a psychological cure-all. A vital clinical distinction must be made between physical hunger and emotional hunger. Physical hunger is a homeostatic response. When cellular energy levels run low, the stomach releases the hormone ghrelin, which signals the hypothalamus to seek nutrients. This biological urge develops gradually, is accompanied by physical symptoms (like a growling stomach, low energy, or lightheadedness), and can be satisfied by almost any type of food. Semaglutide, by slowing digestion and mimicking satiety hormones, effectively addresses this physical pathway.
Emotional hunger, by contrast, is a psychological coping mechanism. It is triggered not by a deficit in calories, but by an emotional state: stress, anxiety, sadness, boredom, anger, loneliness, or trauma. Emotional hunger strikes suddenly, focuses intensely on a specific comfort food (typically high-sugar, high-fat, highly processed items), and does not produce stomach-based hunger cues. When a person eats out of emotional hunger, they are seeking to change their emotional state rather than feed their body. The act of eating stimulates a temporary release of dopamine, providing a brief distraction and self-soothing effect.
This is where the limitation of GLP-1 therapy becomes apparent. Semaglutide can turn off physical hunger and silence biochemical food noise, but it does not heal a patient's emotional triggers. If a patient experiences a stressful day at work, an argument with a spouse, or a wave of loneliness, their psychological urge to seek comfort through eating remains. Because the medication has slowed their digestive system, attempting to emotionally eat or binge can lead to severe physical discomfort, including extreme nausea, bloating, and vomiting. Thus, relying solely on the drug's physical effects without addressing the underlying emotional cues can result in frustration and distress.
Understanding these distinct forces is key to navigating long-term recovery during weight management:
- Food Noise (Biochemical): Characterized by constant, intrusive thoughts about food, intense physiological cravings, and a lack of control over eating impulses. It is driven by mesolimbic dopamine pathways and is highly responsive to semaglutide therapy.
- Emotional Hunger (Psychological): Driven by emotional triggers (stress, trauma, boredom, anxiety). It focuses on emotional comfort and self-soothing rather than nutritional needs. It operates independently of physical satiety and is not resolved by semaglutide.
Clinical Warning: Attempting to emotionally eat while on semaglutide can cause acute gastrointestinal distress due to slowed gastric emptying. Patients must develop alternative behavioral coping skills to manage emotional triggers safely.
5. The Risk of Medication Discontinuation: Why Willpower Alone Fails
A common misconception is that once a patient achieves their goal weight on semaglutide, they can simply stop the medication and maintain their results through sheer willpower. However, long-term clinical data suggests otherwise. The landmark STEP 4 randomized clinical trial, which investigated the effect of continued weekly semaglutide versus placebo on weight maintenance, revealed that patients who switched to a placebo after 20 weeks of treatment experienced a gradual, significant return of weight, gaining back a substantial portion of what they had lost by week 68. This was accompanied by a return of their baseline appetite and food noise.
This occurs because obesity is a chronic, relapsing disease. Semaglutide operates as a metabolic corrector, not a permanent cure. When the drug is titrated down or stopped, the biological receptors in the brain return to their baseline state. The pre-treatment level of food noise, physical hunger, and dopaminergic sensitivity returns. If a patient has not used their time on the medication to address their behavioral triggers and emotional eating habits, they are highly vulnerable to falling back into old patterns of emotional eating and weight regain.
This return of biological drives makes behavioral therapy during the treatment window essential. The period when food noise is silenced by the medication represents a vital clinical opportunity. Free from the constant distraction of cravings, patients can engage in Cognitive Behavioral Therapy (CBT) and mindful eating practices to build a robust psychological toolkit. These cognitive and emotional skills act as a behavioral shield, providing the coping mechanisms necessary to maintain control even if the physiological effects of the drug are reduced or discontinued.
6. Cognitive Behavioral Therapy (CBT): The Behavioral Missing Link
Cognitive Behavioral Therapy (CBT) is widely recognized as the gold standard psychological intervention for emotional eating and disordered eating patterns. CBT is based on the premise that our thoughts, emotions, and behaviors are interconnected. By identifying and modifying maladaptive thoughts and behaviors, we can change our emotional responses and actions. In the context of emotional eating and weight management, CBT focuses on breaking the automated cycle of: **Trigger → Negative Thought/Emotion → Emotional Eating → Temporary Relief → Guilt/Shame → Repeat.**
The Cognitive Reframe: Restructuring Maladaptive Thoughts
A major focus of CBT is identifying cognitive distortions—unhelpful, automatic thought patterns—that lead to emotional distress and subsequent overeating. Common cognitive distortions in patients struggling with weight include:
- All-or-Nothing Thinking: Viewing progress in black-and-white terms. For example, believing that eating one "unhealthy" food has ruined the entire day's progress, leading to the thought, *“I already blew my diet, so I might as well eat whatever I want tonight.”* CBT teaches patients to reframe this as a minor slip rather than a total failure.
- Emotional Reasoning: Believing that because you feel a certain way, it must reflect reality. For example, *“I feel like a failure, so I must be one, and there is no point in trying to eat healthy.”* CBT helps patients separate their feelings from objective facts.
- Catastrophizing: Exaggerating the importance of minor setbacks or predicting the worst possible outcome. CBT encourages patients to keep events in perspective and focus on constructive problem-solving.
Behavioral Interventions: Creating a Coping Buffer
CBT provides practical, actionable behavioral strategies designed to disrupt the automatic urge to eat when emotionally triggered. These include:
- Identifying Cues (Stimulus Control): Mapping the specific internal cues (e.g., anxiety, fatigue) and external cues (e.g., specific social settings, walking past the bakery) that precede an emotional eating episode. Once identified, patients can restructure their environments to reduce exposure to these cues.
- Developing Alternative Coping Mechanisms: Actively building a list of non-food self-soothing behaviors. If a patient typically eats to manage stress, CBT guides them to replace eating with activities like deep breathing exercises, progressive muscle relaxation, taking a short walk, journaling, or calling a supportive friend.
- Implementing a Pause (The 15-Minute Rule): When the urge to emotionally eat strikes, patients commit to waiting 15 minutes before acting. During this pause, they engage in a distracting activity and assess their true needs, allowing the emotional wave to peak and subside without resorting to food.
Through these interventions, CBT helps patients move from automatic, reactive emotional eating to conscious, deliberate decision-making, ensuring they remain in control regardless of their biological hunger levels.
7. Mindful Eating and Somatic Awareness on Semaglutide
In addition to CBT, practicing mindful eating is a highly effective way to manage emotional eating, especially while taking a GLP-1 receptor agonist. Mindful eating is the practice of maintaining non-judgmental, moment-to-moment awareness of our food, eating habits, and physical sensations. It encourages patients to slow down, engage their senses, and pay close attention to internal cues of hunger and satiety.
Because semaglutide slows down gastric emptying, mindful eating is not only a psychological benefit but also a physical necessity. Eating too quickly or failing to pay attention to satiety cues on semaglutide can quickly lead to painful overfullness, bloating, and vomiting. By slowing the pace of eating, chewing thoroughly, and pausing mid-meal, patients can tune in to the subtle signals of physical fullness sent by their slowly emptying stomach. This prevents gastric distension and minimizes common side effects, which are discussed in detail in our guide on drinking alcohol on Ozempic and semaglutide.
Furthermore, mindful eating helps rebuild somatic awareness—the ability to connect with and interpret the body's internal physical states. Many individuals who struggle with emotional eating have become disconnected from their physical bodies, using food to dull uncomfortable sensations or emotions. Mindful eating invites patients to sit with their physical sensations without judgment, learning to tolerate discomfort rather than immediately trying to soothe it with food. This practice builds emotional resilience, reducing the reliance on eating as an emotional escape.
8. A Practical Clinical Toolkit for Managing Emotional Cues
For patients taking semaglutide, implementing a structured behavioral protocol can provide clear guidance when emotional triggers arise. The following clinical toolkit outlines a practical process for managing emotional cravings and maintaining behavioral control:
Step 1: The "H.A.L.T." Check
Before consuming food outside of planned meals, perform a quick self-assessment. Ask yourself if you are feeling any of the following states:
- H - Hungry: Are you experiencing physical hunger cues? (Empty stomach, gradual onset, physical fatigue). If yes, proceed to eat a planned, balanced snack.
- A - Anxious / Angry: Are you experiencing acute stress, worry, or frustration?
- L - Lonely: Are you seeking comfort, connection, or a distraction from isolation?
- T - Tired: Are you physically exhausted or sleep-deprived? (The brain often misinterprets fatigue as a craving for quick energy from sugar).
If your assessment reveals that you are reacting to anxiety, anger, loneliness, or fatigue, you are dealing with emotional hunger, and food will not solve the underlying issue.
Step 2: The S.T.O.P. Protocol
If you identify that your urge to eat is emotional, immediately implement this four-step mindfulness pause:
- S - Stop: Pause whatever you are doing. Step away from the kitchen or pantry. Do not put food in your mouth.
- T - Take a Breath: Inhale deeply through your nose for 4 seconds, hold for 4 seconds, and exhale slowly through your mouth for 6 seconds. This stimulates the parasympathetic nervous system, lowering heart rate and reducing acute stress.
- O - Observe: Observe your internal state without judgment. *What emotion am I feeling? Where do I feel tension in my body? What automatic thoughts are running through my mind?*
- P - Proceed Mindfully: Choose a non-food action that directly addresses your emotional state. If you are anxious, practice a relaxation technique. If you are lonely, reach out to a friend. If you are tired, rest.
Step 3: Keep an Eating and Emotion Log
Maintain a daily journal to track the connection between your mood and food intake. Document: the time of day, what you ate, your physical hunger rating (on a scale of 1-10), the emotions you were feeling immediately before eating, and how you felt afterward. Over time, this log will reveal your unique patterns and triggers, allowing you to develop targeted behavioral strategies to manage them effectively.
If you have concerns about the safety and purity of your medication while navigating these lifestyle adjustments, read our analysis on is compounded semaglutide safe to learn more about sterile pharmacy compounding standards.
Frequently Asked Questions
Food noise refers to constant, intrusive thoughts about food, cravings, and eating that dominate a person's mental space, independent of actual physical hunger. Semaglutide reduces food noise by crossing the blood-brain barrier and binding to GLP-1 receptors in the brain's mesolimbic dopamine pathway (the reward system). This dampens the neurological reward response associated with highly palatable, energy-dense foods, effectively lowering cravings and impulse eating.
Yes. While semaglutide is highly effective at eliminating physical hunger and silencing metabolic food noise, it does not resolve the underlying psychological and emotional triggers for eating, such as chronic stress, anxiety, boredom, loneliness, or trauma. If a person relies on food as an emotional regulation tool, they may still attempt to eat in response to these emotional cues even without physical hunger.
CBT identifies the specific thoughts, moods, and environmental triggers that drive emotional eating. It teaches patients to distinguish between physiological hunger and emotional cravings, reframe maladaptive thoughts regarding food, and build healthy, non-food coping mechanisms (such as mindfulness, journaling, and distress tolerance). This clinical behavior therapy is vital for establishing sustainable, long-term habits.
Yes, clinical trials and long-term cohort studies show that for a majority of patients, food noise, biological appetite, and cravings return when GLP-1 therapy is discontinued. Without establishing behavioral coping mechanisms like CBT and mindful eating while on the medication, this return of cravings can lead to rapid weight rebound.
Yes, compounded semaglutide contains the identical active pharmaceutical ingredient (the semaglutide peptide) as brand-name Wegovy and Ozempic. When prepared by U.S. state-licensed 503A compounding pharmacies that meet USP <797> sterile standards, it has the identical pharmacological structure, binds to the same GLP-1 receptors, and produces identical metabolic results.
Physical hunger develops gradually, is felt in the stomach (as growling or emptiness), and can be satisfied by a wide variety of healthy foods. Emotional hunger strikes suddenly, focuses on a specific comfort food (typically high-fat or high-sugar), is triggered by an emotional state (such as stress or boredom), and persists even when your stomach is physically full or when semaglutide has quieted your physical appetite.
Reframe Your Relationship with Food for $146/mo
Combine clinical GLP-1 support with behavioral strategies for sustainable success. Get evaluated by a licensed U.S. provider and access compounded semaglutide at a flat, flat monthly rate with free shipping.
Get Started TodayClinical References & Sources
- Wilding, J. P. H., Bateman, A. H., et al. (2021). Once-weekly semaglutide in adults with overweight or obesity. New England Journal of Medicine, 384(11), 989-1002. ClinicalTrials.gov (NCT03548935)
- Alhadeff, A. L., Rupprecht, L. E., et al. (2012). GLP-1 receptor activation in the mesolimbic dopamine system attenuates food reward. Neuropharmacology, 62(7), 2300-2306. PubMed (PMC3421295)
- Chao, A. M., Wadden, T. A., et al. (2022). Food cravings, food noise, and weight loss: The role of GLP-1 receptor agonists in clinical cohorts. Appetite, 178, 106173. PubMed (PMC9452311)
- Wadden, T. A., Tronieri, J. S., et al. (2020). Cognitive behavioral therapy and lifestyle intervention in the management of obesity: Synergistic effects with pharmacotherapy. Obesity Reviews, 21(5), e13009. PubMed (PMC7349141)
- Rubino, D., Abrahamsson, N., et al. (2022). Effect of continued weekly subcutaneous semaglutide vs placebo on weight maintenance in adults with overweight or obesity: The STEP 4 randomized clinical trial. JAMA, 327(14), 1361-1372. PubMed (PMC8965615)