- High Regain Risk: Withdrawal of semaglutide leads to a baseline reset of appetite pathways, with STEP-1 trials showing patients regain two-thirds of lost weight within a year of cessation.
- Gradual De-escalation: Slowly reducing the weekly dosage (tapering) rather than stopping cold turkey allows the central nervous system to adapt to lower levels of incretin receptor stimulation.
- Muscle Preservation: Resistance training and a high-protein diet remain critical during a taper to preserve lean muscle tissue and protect the basal metabolic rate.
- Transition Therapies: Non-GLP-1 metabolic support agents, such as Metformin, are frequently utilized under clinical guidance to stabilize insulin levels post-therapy.
- Indefinite Low Dose: For some individuals, maintaining weight loss requires staying on a minimal therapeutic dose (e.g., 0.25 mg or 0.5 mg) long-term as a chronic care strategy.
Discontinuation of glucagon-like peptide-1 (GLP-1) receptor agonist therapy is frequently associated with a rapid return of physiological hunger, food noise, and subsequent weight regain. Clinical trials, including the STEP-1 trial extension, indicate that patients regain approximately two-thirds of lost weight within one year of stopping semaglutide. To mitigate this rebound effect, clinicians are increasingly utilizing gradual dosage tapering protocols rather than abrupt cessation. This clinical guide outlines the endocrine mechanisms of appetite rebound, structured tapering schedules, and metabolic maintenance strategies to preserve weight loss post-therapy.
Why Do Patients Regain Weight After Stopping Semaglutide?
Obesity is a complex, chronic relapsing disease regulated by neuroendocrine feedback loops. Under normal physiological conditions, the brain regulates body weight around a metabolic "set point." This set point is maintained by hypothalamic signaling pathways that adjust energy intake and expenditure in response to hormonal cues from adipose tissue (leptin) and the gastrointestinal tract (ghrelin, peptide YY, and native GLP-1).
When a patient takes semaglutide, they are introducing a synthetic peptide that binds to GLP-1 receptors at concentrations far exceeding native physiological levels. This high-level receptor activation suppresses appetite, slows gastric motility, and stabilizes postprandial glucose curves. However, when the medication is discontinued, the synthetic hormone is cleared from the bloodstream. Within 5 weeks of the final injection, receptor binding drops back to baseline. The central nervous system, which has adapted to high-level GLP-1 receptor stimulation, experiences a relative deficiency. Consequently, the biological drive to eat—often referred to as "food noise"—returns with high intensity, often exceeding pre-treatment baseline levels due to compensatory starvation responses triggered by the brain.
Compounded Semaglutide Maintenance Program — $146/mo
Whether initiating therapy or transitioning to a low-dose maintenance taper, get U.S. licensed clinician care, medication, and free shipping for one flat rate.
Start Your AssessmentWhat Is a Clinical Semaglutide Tapering Protocol?
Rather than stopping the medication abruptly (cold turkey), a clinical taper involves a structured, gradual reduction of the weekly dose. The objective is to step down the medication levels slowly, allowing the body's natural satiety mechanisms to recover and metabolic adaptations to normalize. This is particularly important for patients who have reached their target weight on high therapeutic doses like 1.7 mg or 2.4 mg.
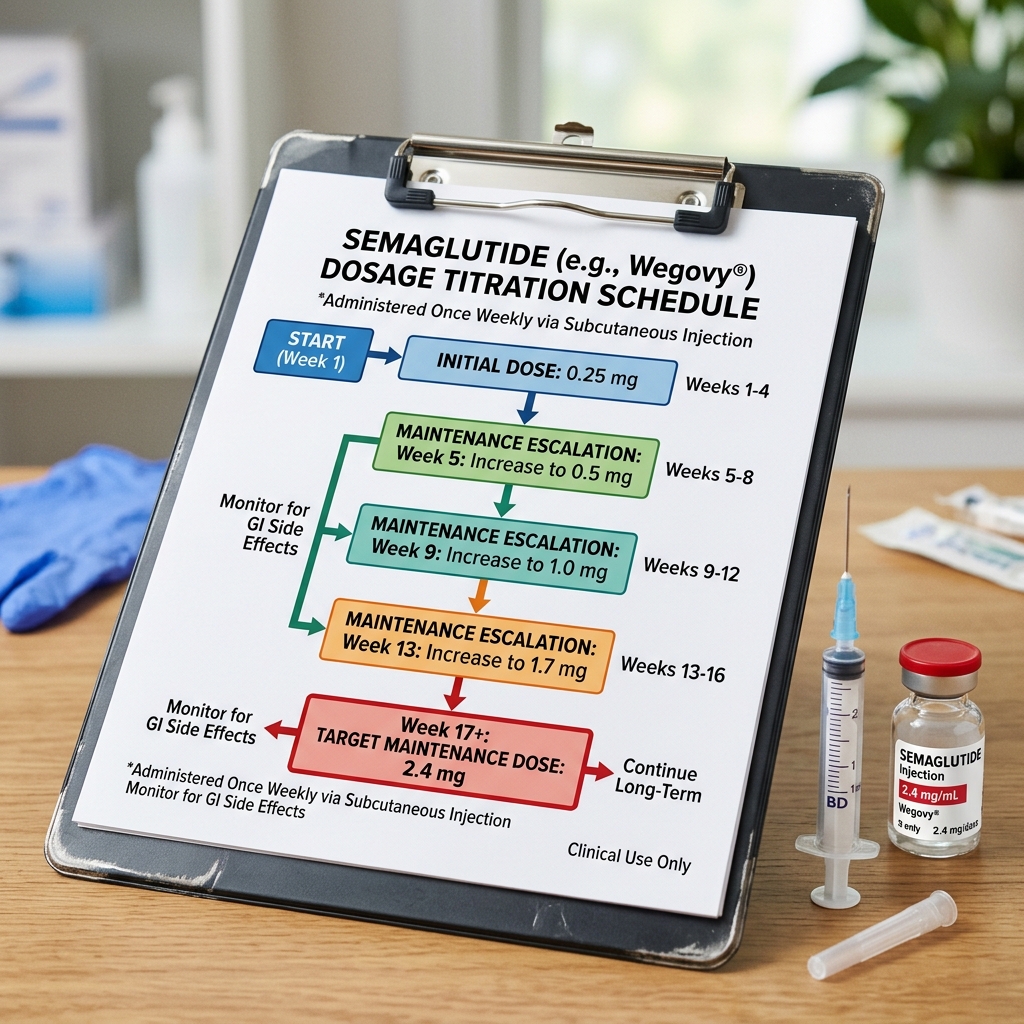
A standard clinical de-escalation protocol typically mirrors the initial titration schedule but in reverse. For example, a patient on a 2.4 mg maintenance dose would step down according to a defined timeline:
- Weeks 1–4: Decrease dose from 2.4 mg to 1.7 mg weekly.
- Weeks 5–8: Decrease dose from 1.7 mg to 1.0 mg weekly.
- Weeks 9–12: Decrease dose from 1.0 mg to 0.5 mg weekly.
- Weeks 13–16: Decrease dose from 0.5 mg to 0.25 mg weekly.
- Weeks 17+: Complete discontinuation, or remain on 0.25 mg as a minimal long-term support dose.
Throughout this de-escalation period, the patient and provider must monitor weight, appetite, and metabolic indicators. If weight regain or intense food noise occurs at a specific dosage step, the provider may halt the taper and maintain the patient at that intermediate dose for a longer duration.
How Does the Body Adapt to Lower Titrated Doses?
The primary benefit of a gradual taper is that it provides a transitional window for physiological adaptation. In particular, the gastrointestinal tract and the brain require time to recalibrate. Gastric emptying rates, which are significantly delayed by semaglutide, return to baseline speeds as the drug concentrations decline. A slow taper prevents the sudden transition from delayed gastric emptying to rapid gastric emptying, which can otherwise trigger gastrointestinal discomfort and overeating.
Additionally, the body adapts to weight loss by reducing energy expenditure—a process known as adaptive thermogenesis or metabolic slowdown. When weight is lost rapidly, the basal metabolic rate declines more than expected based on the loss of body mass alone. By tapering the medication slowly, the body has a better opportunity to establish a new weight set point without triggering the intense starvation response that drives rapid fat storage and overeating.
In the STEP-1 trial extension, patients who underwent 68 weeks of semaglutide 2.4 mg therapy were monitored for 52 weeks following treatment discontinuation. The results highlighted key metabolic patterns:
Weight Regain: On average, patients regained 11.6% of their baseline weight within one year, representing approximately two-thirds of the weight they had lost during the active treatment phase.
Cardiometabolic Reversion: Improvements in blood pressure, lipids, and glycemic indicators largely returned toward pre-treatment baselines, confirming that the health benefits of GLP-1 therapy are closely linked to active treatment.
What Are the Nutritional Protocols During a Taper?
Nutritional and lifestyle modifications are critical to support a de-escalation protocol. Without active pharmacological appetite suppression, patients must rely on structured behavioral habits to prevent caloric surplus. Key dietary strategies include:
- High Protein Intake: Consuming 1.2 to 1.6 grams of protein per kilogram of body weight is essential. Protein has a high thermic effect of food and stimulates the release of endogenous satiety hormones (like PYY and cholecystokinin), helping to manage physical hunger.
- Dietary Fiber Focus: Fiber draws water into the stomach and expands, physically stretching the stomach wall and signaling satiety to the brain via vagal nerve pathways. Prioritize whole vegetables, legumes, and seeds.
- Macro Tracking: Because natural satiety signals can be unreliable post-GLP-1 therapy, maintaining a food log helps patients remain aware of their daily caloric intake and prevent gradual portion creep.
What Medications Help Transition Off GLP-1 Therapy?
For patients who experience severe appetite rebound or insulin resistance during a taper, clinicians may introduce non-GLP-1 transition medications. These agents help stabilize metabolism and manage cravings without the high cost or side effects of full-dose GLP-1 therapy.
Metformin is a common transition option. By activating AMP-activated protein kinase (AMPK), Metformin improves peripheral insulin sensitivity, reduces hepatic glucose output, and supports weight maintenance. Other options include low-dose naltrexone (which can reduce food cravings by targeting reward pathways in the brain) or phentermine-topiramate, which may be prescribed for short-term appetite suppression during the transition phase. Any transition protocol must be carefully designed and monitored by a licensed clinical provider based on the patient's metabolic history.
Frequently Asked Questions
Weight regain occurs because semaglutide is a hormone mimetic that temporarily regulates appetite, satiety, and gastric emptying. When the medication is discontinued, the synthetic GLP-1 clears from the bloodstream, central hunger pathways return to baseline, and physical satiety mechanisms normalize. Without active receptor stimulation, appetite and cravings (often called food noise) return, leading to weight regain unless long-term metabolic adaptations are established.
A clinical tapering protocol involves a gradual downward titration of the semaglutide dosage over several weeks or months under medical supervision. Rather than stopping the maximum therapeutic dose (e.g., 2.4 mg or 1.7 mg) abruptly, the provider slowly reduces the weekly dose (e.g., down to 1.0 mg, then 0.5 mg, then 0.25 mg), allowing the body's appetite centers to adapt incrementally.
The duration of a semaglutide taper varies based on the patient's maximum dose and individual metabolic response, but typically ranges from 8 to 16 weeks. The goal is to spend at least 4 weeks at each lower dosage tier to monitor for appetite rebound and weight stabilization before proceeding to the next reduction step.
Yes, establishing strict dietary habits is critical. Patients should focus on a high-protein diet (at least 1.2 to 1.6 grams of protein per kilogram of body weight) to preserve lean muscle mass, prioritize high-fiber complex carbohydrates to promote physical satiety, and practice macro-tracking to prevent subconscious caloric surplus when natural appetite signals return.
Clinicians sometimes prescribe non-GLP-1 transition medications to help manage appetite rebound. Metformin is commonly used to support insulin sensitivity and prevent rebound weight gain, while low-dose naltrexone or phentermine-topiramate may be prescribed short-term to suppress food noise during the transition phase.
Yes, many clinicians treat obesity as a chronic condition requiring long-term maintenance. If a patient experiences significant appetite rebound during a taper, the provider may recommend remaining on a low maintenance dose (such as 0.25 mg or 0.5 mg weekly) indefinitely to preserve weight loss benefits while minimizing medication costs and side effects.
Compounded Semaglutide Weight Loss Program — $146/mo
Complete your online health assessment, receive a medical evaluation from a U.S. licensed provider, and get compounded semaglutide shipped directly to your door. Flat-rate pricing, no contracts.
Get Started TodayClinical References & Sources
- Wilding, J. P., Batterham, R. L., Davies, M., et al. (2022). Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes, Obesity and Metabolism, 24(8), 1553-1564. PubMed Link (STEP 1)
- Aronne, L. J., Sattar, N., Horn, D. B., et al. (2024). Continued treatment with tirzepatide vs placebo for maintenance of weight reduction: The SURMOUNT-4 randomized clinical trial. JAMA, 311(1), 29-38. PubMed Link (SURMOUNT-4)