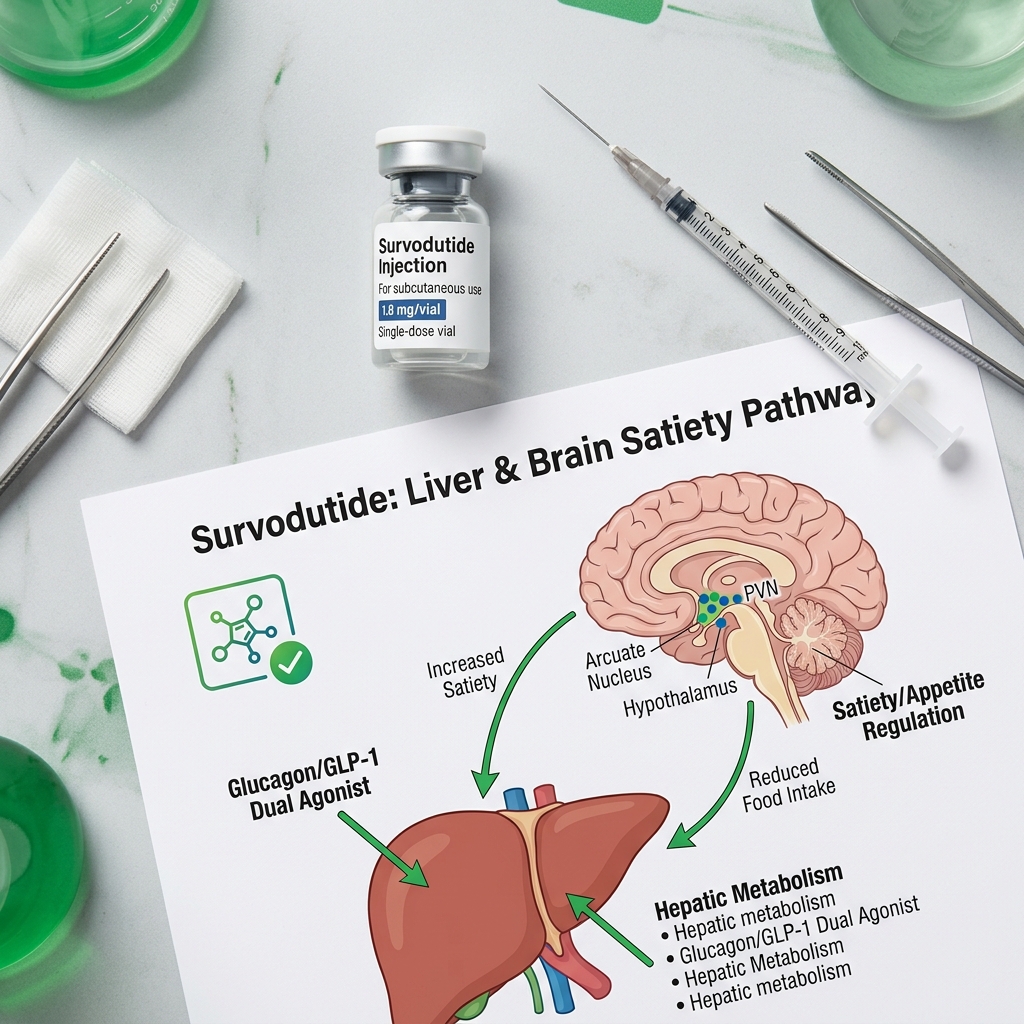
- Dual Glucagon/GLP-1 Mechanism: Survodutide targets both GLP-1 and glucagon receptors. GLP-1 reduces food intake and gastrointestinal transit, while glucagon increases resting energy expenditure and directly triggers hepatic lipid oxidation.
- Phase 2 Weight Loss Efficacy: Published clinical trial data (Zimmerman et al., 2023) demonstrated that adults with overweight or obesity achieved up to 18.7% (often rounded to 19%) mean body weight reduction over 46 weeks at the highest therapeutic dose.
- Histological MASH Breakthrough: A landmark NEJM study (Sanyal et al., 2024) demonstrated that up to 83% of patients with metabolic dysfunction-associated steatohepatitis (MASH) and stage F1-F3 fibrosis achieved significant histological resolution without worsening fibrosis.
- Active Phase 3 Pipeline: The SYNCHRONIZE global trials (SYNCHRONIZE-1 and -2) are currently ongoing to assess the long-term safety, cardiovascular outcomes, and sustained efficacy of survodutide in larger populations.
- Standard Incretin Side Effects: Tolerability concerns match traditional GLP-1 therapies, characterized primarily by mild-to-moderate transient gastrointestinal adverse events (nausea and vomiting) during dose escalation.
- Projected FDA Timeline: With Phase 3 trials progressing rapidly, regulatory submissions are anticipated to lead to an estimated FDA approval window in late 2026 or during 2027.
Introduction: The Expansion of Receptor-Targeted Weight Wellness
The therapeutic paradigm for obesity has undergone a rapid evolution over the past decade. The clinical success of single-receptor glucagon-like peptide-1 (GLP-1) agonists, such as semaglutide, established that gut hormones could be harnessed to achieve significant, sustained body weight reduction. This was soon followed by dual GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) agonists like tirzepatide, which demonstrated that targeting multiple metabolic pathways could lead to even greater weight loss. Today, the frontier of metabolic medicine has expanded to include co-agonists that target the glucagon receptor alongside GLP-1. At the center of this research is survodutide (formerly BI 456906), a dual GLP-1/glucagon receptor agonist co-developed by Boehringer Ingelheim and Zealand Pharma.
Unlike therapies that focus solely on suppressing appetite, survodutide represents a physiological shift by combining calorie reduction with increased energy expenditure. By activating the glucagon receptor, this compound stimulates hepatic lipid metabolism and elevates resting metabolic rate, while its GLP-1 component manages satiety and controls glycemia. This combination has shown promise not only for chronic weight management but also as a potential treatment for metabolic dysfunction-associated steatohepatitis (MASH), a progressive liver disease closely linked to obesity. In this clinical guide, we will analyze the biochemical pathways of survodutide, examine the data from its Phase 2 weight loss and MASH clinical trials, outline the active Phase 3 SYNCHRONIZE trial program, and review its expected FDA approval timeline.
The Dual-Target Mechanism: Apppetite Control and Metabolic Activation
To understand why survodutide is generating significant clinical interest, it is necessary to examine the biological roles of GLP-1 and glucagon. Traditional weight loss medications operate primarily by reducing energy intake. Survodutide is a single peptide backbone designed to bind to and activate both the GLP-1 receptor (GLP-1R) and the glucagon receptor (GCGR) simultaneously, balancing appetite suppression with metabolic stimulation.
1. GLP-1 Receptor Agonism: Appetite Suppression & Gastric Delay
Glucagon-like peptide-1 is an incretin hormone secreted by the L-cells of the distal gut in response to nutrient ingestion. Its primary metabolic actions include:
- Satiety Induction: GLP-1 crosses the blood-brain barrier to target POMC/CART neurons in the arcuate nucleus of the hypothalamus. This suppresses hunger signals and reduces central "food noise" (intrusive cravings).
- Gastric Retardation: By slowing gastric emptying, GLP-1 prolongs postprandial gut distension. This physical effect sends sustained vagal nerve signals to the brain, maintaining a feeling of fullness for longer periods.
- Glycemic Control: GLP-1 stimulates insulin release from pancreatic beta cells in a glucose-dependent manner while inhibiting glucagon release from alpha cells under hyperglycemic conditions, preventing blood glucose spikes.
This pathway is the foundation of established therapies like semaglutide. For more details on this mechanism, you can read our complete guide to semaglutide.
2. Glucagon Receptor Agonism: Thermogenesis & Hepatic Lipid Oxidation
Glucagon has historically been viewed primarily as a counter-regulatory hormone that raises blood glucose levels during hypoglycemia by promoting hepatic glycogenolysis and gluconeogenesis. However, recent endocrinological research has highlighted glucagon's role in energy balance and lipid homeostasis when activated alongside GLP-1. Its primary metabolic pathways include:
- Resting Energy Expenditure (REE): Glucagon stimulates mitochondrial oxidative phosphorylation and thermogenesis, particularly in brown adipose tissue (BAT). This increases the number of calories the body burns at rest.
- Hepatic Fat Clearance: Glucagon directly targets liver cells, promoting beta-oxidation (the breakdown of fatty acids) and inhibiting lipogenesis (the synthesis of new fat). This helps clear accumulated intracellular lipids from hepatocytes.
- Lipolysis Activation: Glucagon stimulates hormone-sensitive lipase in white adipose tissue, promoting the mobilization of stored triglycerides into free fatty acids to be used for energy.
The Synergy of Co-Agonism
Historically, using glucagon alone for weight loss was limited because its glucose-raising effects could worsen insulin resistance or trigger hyperglycemia in patients with pre-existing metabolic dysfunction. Survodutide addresses this challenge by combining glucagon receptor activation with GLP-1 receptor activation. The GLP-1 component enhances insulin secretion and improves peripheral insulin sensitivity, offsetting the glucose-raising effects of glucagon. Meanwhile, both hormones work together to suppress appetite, while the glucagon pathway helps maintain energy expenditure during calorie restriction, helping to prevent the metabolic slowdown that often occurs during weight loss.
Clinical Insight: In addition to its metabolic and thermogenic effects, glucagon contributes directly to satiety through pathways separate from GLP-1. When glucagon activates hepatic glucagon receptors, it initiates a signaling cascade that travels via the vagus nerve to the solitary tract in the brainstem. This hepatic-portal sensory pathway helps signal nutritional fullness to the brain, complementing the hypothalamic actions of GLP-1 to suppress appetite through two distinct physiological routes.
Phase 2 Weight Loss Results: Zimmerman et al. (2023)
The clinical efficacy of survodutide for weight loss was first documented in a randomized, double-blind, placebo-controlled Phase 2 dose-finding trial published in The Lancet (Zimmerman et al., 2023). This trial evaluated the efficacy and safety of survodutide in adults with obesity or overweight over a 46-week treatment period.
Trial Design and Methodology
The study enrolled adults with a body mass index (BMI) of 30 kg/m² or higher, or a BMI of 27 kg/m² or higher with at least one weight-related comorbidity (such as dyslipidemia, hypertension, or sleep apnea), excluding patients with type 2 diabetes. A total of 387 participants were randomized to receive weekly subcutaneous injections of either survodutide (in dose-escalation cohorts of 0.6 mg, 2.4 mg, 3.6 mg, or 4.8 mg) or a placebo. The trial lasted 46 weeks, consisting of a 20-week dose-escalation phase followed by a 26-week stable maintenance phase.
Weight Loss Outcomes
Survodutide demonstrated significant, dose-dependent reductions in body weight at week 46:
- The 4.8 mg Cohort: Participants randomized to the highest dose achieved a mean body weight reduction of 14.9% in the primary intention-to-treat analysis. Among those who successfully tolerated and remained on the maximum 4.8 mg dose throughout the study, the average weight loss reached 18.7% (often rounded to 19% in clinical summaries).
- The 3.6 mg Cohort: Participants in this cohort achieved an average weight loss of 13.6% by week 46.
- The 2.4 mg Cohort: This group showed an average body weight reduction of 12.1%.
- The Placebo Cohort: Participants receiving the placebo achieved an average weight loss of 2.8%.
Additionally, a significant proportion of participants in the higher-dose groups achieved key clinical weight loss milestones. In the 4.8 mg group, approximately 67% of participants lost 10% or more of their baseline body weight, and 40% achieved a weight loss of 15% or more, compared to 26% and 10% in the placebo group, respectively.
Efficacy Trajectory
A notable finding from the Phase 2 trial was the trajectory of the weight loss curve. At week 46, the weight loss curve for the higher survodutide doses had not plateaued. This suggests that the full therapeutic potential of the drug may not have been reached by week 46, and that longer treatment durations—such as the 80-week periods being evaluated in the Phase 3 trials—could yield additional weight reduction.
| Medication | Receptor Targets | Trial Duration | Mean Weight Loss | Primary Clinical Trial |
|---|---|---|---|---|
| Semaglutide (Wegovy) | GLP-1 Only | 68 Weeks | 14.9% - 15.0% | STEP-1 (Wilding et al., 2021) |
| Tirzepatide (Zepbound) | GLP-1 + GIP | 72 Weeks | 20.9% | SURMOUNT-1 (Jastreboff et al., 2022) |
| Survodutide (BI 456906) | GLP-1 + Glucagon | 46 Weeks (Phase 2) | Up to 18.7% / 19.0% | Lancet Phase 2 (Zimmerman et al., 2023) |
| Retatrutide | GLP-1 + GIP + Glucagon | 80 Weeks (Phase 3) | 28.3% | TRIUMPH-1 (Lilly Press Release, 2026) |
Hepatic and MASH Benefits: Sanyal et al. (2024)
Beyond weight loss, survodutide's glucagon component makes it a potential candidate for treating liver diseases associated with metabolic syndrome. Metabolic dysfunction-associated steatohepatitis (MASH), formerly known as non-alcoholic steatohepatitis (NASH), is characterized by fat accumulation in the liver, cell injury, and inflammation, which can progress to liver fibrosis, cirrhosis, and hepatic failure. The clinical efficacy of survodutide in MASH was evaluated in a randomized Phase 2 trial published in the New England Journal of Medicine (Sanyal et al., 2024).
MASH Trial Design
The 48-week randomized, double-blind, placebo-controlled trial enrolled 295 adults with biopsy-confirmed MASH and moderate-to-severe liver fibrosis (stages F1, F2, or F3). Participants were randomized to receive weekly subcutaneous doses of survodutide (2.4 mg, 4.8 mg, or 6.0 mg) or a placebo. The primary endpoint was histological improvement in MASH (resolution of steatohepatitis) without worsening of fibrosis at week 48, assessed by liver biopsies before and after the treatment period.
Key Findings
The trial met its primary endpoint, demonstrating significant histological improvement in MASH:
- Significant MASH Improvement: Up to 83.0% of patients treated with survodutide achieved MASH resolution without worsening of fibrosis, compared to 18.2% of patients in the placebo group. This response rate was statistically significant across all evaluated doses (2.4 mg, 4.8 mg, and 6.0 mg).
- Relative Hepatic Fat Reduction: Secondary endpoints showed a dose-dependent reduction in liver fat content, measured by magnetic resonance imaging proton density fat fraction (MRI-PDFF). Patients in the survodutide groups experienced relative liver fat reductions of up to 64.3%, compared to minor changes in the placebo group.
- Fibrosis Stabilization and Regression: A secondary endpoint evaluated the percentage of patients achieving an improvement in fibrosis by at least one stage without worsening of MASH. In the survodutide groups, up to 34.5% of patients achieved fibrosis regression, compared to 20.8% in the placebo group. Crucially, the trial showed that survodutide treatment did not worsen fibrosis in the vast majority of patients.
Clinical Significance
These histological findings suggest that survodutide's glucagon receptor activation helps clear hepatic lipids, which may reduce lipotoxicity and subsequent inflammatory damage in the liver. While several GLP-1 receptor agonists have shown indirect benefits on liver fat by promoting general weight loss, survodutide's direct targeting of hepatic lipid pathways via the glucagon receptor may offer a more direct mechanism for treating MASH. This has positioned survodutide as a potential therapeutic option in both metabolic hepatology and obesity medicine.
Access Compounded GLP-1 Therapy Online — From $146/mo
While next-generation dual agonists like survodutide complete clinical development, you can start a weight loss program today. Get prescribed compounded Semaglutide or Tirzepatide by U.S. licensed providers, shipped to your door.
Start Your AssessmentThe Phase 3 SYNCHRONIZE Trials: Long-Term Safety and Efficacy
Building on the Phase 2 results, Boehringer Ingelheim and Zealand Pharma initiated a global Phase 3 clinical trial program known as SYNCHRONIZE. This program is designed to confirm the long-term safety, tolerability, and efficacy of survodutide across diverse patient populations.
SYNCHRONIZE-1 (NCT06066112)
This randomized, double-blind, placebo-controlled trial is evaluating survodutide in adults with obesity or overweight (BMI ≥ 30 kg/m², or ≥ 27 kg/m² with weight-related comorbidities) who do not have type 2 diabetes. The study is assessing change in body weight over a longer period (typically 76 to 80 weeks) to determine if extending treatment beyond the 46 weeks of Phase 2 leads to additional weight loss and to evaluate long-term safety.
SYNCHRONIZE-2 (NCT06076577)
This trial is evaluating the efficacy, safety, and tolerability of survodutide in adults with obesity or overweight who also have type 2 diabetes. Because patients with diabetes historically experience slower weight loss on incretin therapies, this trial will provide data on how the dual-agonist pathway performs in this population and assess its impact on glycemic control (HbA1c levels).
SYNCHRONIZE-CVOT and Hepatic Trials
Additional trials within the SYNCHRONIZE program are evaluating cardiovascular outcomes (CVOT) to assess the drug's safety profile in patients at high risk for cardiovascular events, as well as its impact on kidney function. Ongoing trials are also further evaluating survodutide in patients with biopsy-confirmed MASH to monitor long-term histological changes and assess the durability of hepatic fat clearance.
Side Effects and Tolerability: Mitigating Gastrointestinal Events
While the clinical data shows significant efficacy, evaluating next-generation therapies requires assessing their safety and tolerability profiles. In trials completed to date, survodutide's safety profile has been generally consistent with the incretin class, but glucagon receptor activation introduces unique physiological considerations.
1. Gastrointestinal Adverse Events
As with all GLP-1 receptor agonists, the most common side effects reported in survodutide trials are gastrointestinal. These include:
- Nausea: The most frequently reported adverse event, typically occurring during the dose-escalation phase.
- Vomiting: Reported primarily during rapid dose increases, generally resolving once a stable maintenance dose is reached.
- Diarrhea & Constipation: Common mild-to-moderate GI side effects, consistent with slowed gastrointestinal transit.
In the Phase 2 obesity trial, these side effects were mostly mild-to-moderate and occurred primarily during the 20-week dose-escalation phase. However, because of the drug's dual potency, rapid titration was associated with higher rates of treatment discontinuation. This highlights the clinical importance of slow, progressive dose titration.
2. Heart Rate and Blood Pressure Profiles
Due to the presence of glucagon receptors in the sinoatrial node of the heart, glucagon receptor activation can lead to changes in heart rate. In clinical trials, participants receiving higher doses of survodutide experienced a mild, transient increase in resting heart rate (typically an average of 2 to 4 beats per minute), which generally stabilized over time. Clinicians monitor these cardiac vital signs, particularly in patients with pre-existing cardiovascular conditions, as part of the ongoing safety assessments in the SYNCHRONIZE program.
3. Dose Titration Protocol
To improve tolerability and minimize gastrointestinal side effects, the Phase 3 trials utilize a gradual dose-escalation schedule. Patients start on a low initial dose (e.g., 0.6 mg once weekly) and gradually titrate upward at monthly intervals to higher maintenance doses. This step-wise approach allows the gastrointestinal system and cardiovascular pathways to adapt to the medication, helping to lower discontinuation rates and improve patient adherence.
FDA Approval Timeline: Expected Filing and Release Dates
Because survodutide is currently undergoing Phase 3 clinical evaluation, it is not yet approved by the U.S. Food and Drug Administration (FDA) or available for commercial prescription. However, we can project a regulatory timeline based on trial progress and typical FDA review cycles.
Phase 3 Data Compilation (Late 2025 / Early 2026)
The primary trials in the SYNCHRONIZE program are expected to complete their active treatment phases and compile safety data by late 2025 or early 2026. Boehringer Ingelheim and Zealand Pharma will need to audit this data, compile the clinical study reports, and submit a New Drug Application (NDA) to the FDA for chronic weight management and potentially MASH.
FDA Review Cycle (Estimated Late 2026 / 2027)
Once the FDA accepts the NDA filing, it typically takes 10 to 12 months to complete its review under standard timelines. If the FDA grants Priority Review—which could occur for the MASH indication if it is deemed to fill an unmet medical need—the review period could be reduced to 6 months. Based on these factors, the estimated **regulatory approval window for survodutide is projected for late 2026 or during 2027**.
Following approval, commercial launch typically occurs within 30 to 90 days. Patients can expect the medication to become available in retail pharmacies shortly after approval, assuming no manufacturing scale-up delays or supply chain constraints, which have occasionally affected previous launches in the GLP-1 class.
Clinical Positioning: Wegovy vs. Survodutide
As next-generation dual and triple agonists move closer to approval, clinicians will need to determine how to position these therapies relative to existing options like semaglutide (Wegovy) and tirzepatide (Zepbound).
- Single Receptor Agonists (Semaglutide): Semaglutide remains a first-line option for patients seeking a established safety profile and moderate weight loss (average 15%). It is also widely accessible through compounded formulations for patients paying out-of-pocket. For information on costs and insurance coverage, see our guide on Wegovy cost with and without insurance.
- Dual GLP-1/Glucagon Agonists (Survodutide): Survodutide may be preferred for patients with concurrent metabolic dysfunction-associated steatohepatitis (MASH) or significant hepatic steatosis, where the glucagon component can directly target liver fat. It may also serve as an alternative for patients who have plateaued on single GLP-1 therapies.
For patients navigating today's options, understanding the cost landscape is important. You can find detailed information in our review of the cheapest semaglutide online in 2026.
Navigating Weight Management in 2026: Dangers of Research Peptides
Because survodutide is not currently FDA-approved, it is not available for prescription outside of clinical trials. This lack of availability has contributed to the growth of an unregulated online market for "research peptides."
The Risks of Unregulated Peptides
Some online chemical suppliers sell powders labeled as "Survodutide" or "BI 456906" marked "for research use only." These products bypass FDA oversight and pharmacy regulations. Injecting these compounds carries significant health risks:
- Lack of Sterility: Research chemicals are not manufactured in sterile facilities. Injecting non-sterile solutions can lead to serious infections, injection site abscesses, or systemic sepsis.
- Dosing Inconsistencies: Third-party testing of research peptides frequently reveals significant variance in purity and dosage, with some vials containing incorrect doses or active contaminants.
- Unknown Additives: These powders may contain residual chemical solvents, heavy metals, or synthesis byproducts that present toxicity risks.
Safe & Accessible Alternatives Today
Patients seeking weight management support do not need to wait for next-generation approvals or risk their health with unregulated research chemicals. Licensed telehealth platforms like Losing Weight RX provide access to established, compounded GLP-1 therapies:
- Compounded Semaglutide: Offers an affordable weight management option starting at a flat rate of $146/month, prepared by state-licensed 503A compounding pharmacies using sterile compounding standards.
- Compounded Tirzepatide: Provides access to the dual GIP/GLP-1 pathway for patients seeking additional glycemic and weight support under clinical supervision.
Frequently Asked Questions
Survodutide (co-developed by Boehringer Ingelheim and Zealand Pharma) is a dual receptor agonist that targets both GLP-1 and glucagon receptors. The GLP-1 component suppresses appetite, reduces food noise, and slows gastric emptying. The glucagon component increases energy expenditure (metabolic rate) and directly stimulates hepatic fat metabolism, leading to liver fat clearance and enhanced weight loss.
In the Phase 2 trial published in The Lancet (Zimmerman et al., 2023), participants with obesity or overweight achieved up to 18.7% (often rounded to 19%) mean body weight reduction at week 46 when taking the highest dose of survodutide (4.8 mg once weekly). The weight loss curve had not plateaued at week 46, suggesting further reduction with longer duration.
In a Phase 2 trial published in the New England Journal of Medicine (Sanyal et al., 2024), up to 83% of patients with MASH and stage F1-F3 fibrosis achieved significant histological resolution without worsening of their fibrosis when treated with survodutide, driven by the glucagon pathway directly reducing liver fat content.
The Phase 3 clinical development program, known as the SYNCHRONIZE trials (including SYNCHRONIZE-1 and SYNCHRONIZE-2), is currently active. These trials are evaluating the long-term safety, tolerability, and weight loss efficacy of survodutide in larger, diverse patient populations over longer treatment durations.
Like other GLP-1 receptor agonists, the most common side effects of survodutide are gastrointestinal, including nausea, vomiting, diarrhea, and constipation. These side effects occur primarily during the dose-escalation phase and are typically mild to moderate. Gradual dose titration is used in trials to improve tolerability.
Regulatory submission is anticipated upon the completion of the Phase 3 SYNCHRONIZE trials, with the projected FDA approval and market release timeline estimated for late 2026 or during 2027, depending on regulatory review timelines.
Start Compounded Semaglutide at $146/mo — Prescribed Online by Licensed Providers
Complete your online assessment, get evaluated by a U.S. licensed provider, and receive compounded semaglutide from a state-licensed 503A compounding pharmacy — shipped directly to your door.
Get Started TodayClinical References & Sources
- Sanyal, A. J., Bedossa, P., Fraessdorf, M., et al. (2024). A Phase 2 randomized trial of survodutide in MASH and fibrosis. New England Journal of Medicine, 391(4), 311-319. PubMed Link
- Zimmerman, R., et al. (2023). Efficacy and safety of survodutide (BI 456906) in adults with overweight or obesity: a randomised, double-blind, active-controlled Phase 2 trial. The Lancet, 402(10405), 879-890. Lancet Link
- Boehringer Ingelheim. (2023). Boehringer Ingelheim and Zealand Pharma initiate Phase III trials for survodutide in obesity. Press Release. Boehringer Ingelheim Newsroom